In the landscape of herbal substances that blur the line between botanical remedy and controlled drug, few have generated as much scientific curiosity, political controversy, and passionate public debate as kratom. Whether you’ve heard of it from a chronic pain forum, a biohacking podcast, or a news headline about federal regulation, there’s more to this Southeast Asian leaf than most people realize, and the story of how it nearly became federally banned tells us something important about the power of informed citizens to shape public health policy.
From Jungle Leaf to American Shelves
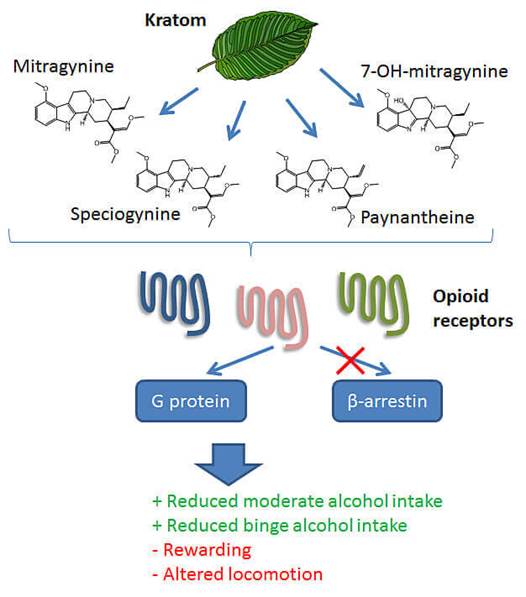
Kratom comes from Mitragyna speciosa, a tropical tree in the coffee family (Rubiaceae) native to Southeast Asia — particularly Thailand, Malaysia, Indonesia, and Papua New Guinea. For centuries, laborers in these regions chewed the leaves to combat fatigue, manage pain, and increase productivity in grueling agricultural conditions. It was folk medicine in the truest sense: low-tech, locally sourced, and passed down through generations.
Today, kratom arrives in American homes as a powder, capsule, or extract — a far cry from fresh-chewed leaves, but the same basic chemistry underneath.
The Chemistry: Two Alkaloids Doing Heavy Lifting
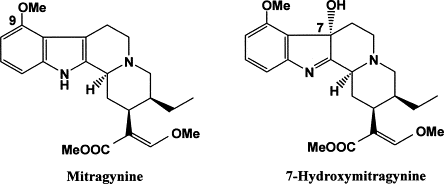
The pharmacological story of kratom centers on its two primary bioactive alkaloids: mitragynine and 7-hydroxymitragynine. Together, these compounds account for the vast majority of kratom’s effects. Mitragynine makes up roughly 60–70% of the total alkaloid content, while 7-hydroxymitragynine is present in much smaller quantities — but is considerably more potent.
Both compounds are indole-based alkaloids with structural features that allow them to interact with opioid receptors in the human brain and body. Their chemical architecture gives them the ability to fit into receptor binding pockets in ways that produce opioid-like effects, though they are structurally distinct from classical opioids like morphine or oxycodone.
How It Works: Mu Receptors, G-Proteins, and a Key Divergence
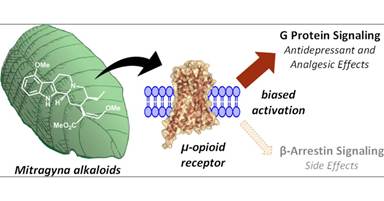
To understand what kratom does in the body, you need a quick primer on opioid receptor pharmacology. The mu-opioid receptor (MOR) is the primary target for most pain-relieving and euphoria-producing opioids. When a drug like morphine binds to the MOR, it triggers two main downstream pathways: one involving G-proteins and another involving molecules called beta-arrestins.
The G-protein pathway is largely responsible for the desirable effects — analgesia, sedation, and euphoria. The beta-arrestin pathway, by contrast, is associated with many of the problematic consequences of opioid use: respiratory depression, tolerance, and constipation.
Here is where kratom’s alkaloids get genuinely interesting from a pharmacological standpoint. Both mitragynine and 7-hydroxymitragynine are partial agonists at the mu-opioid receptor, activating it through G-protein signaling — but critically, they appear to show biased agonism, meaning they activate the G-protein pathway while having relatively little activity at the beta-arrestin pathway. This property, known as “G-protein bias,” is the same pharmacological quality that researchers have been chasing for years in the development of “safer” opioid painkillers. The theory is that a G-protein biased opioid agonist could provide pain relief and mood elevation with a reduced risk of the dangerous side effects tied to beta-arrestin signaling, particularly respiratory depression — the mechanism by which opioid overdoses become fatal.
This does not make kratom safe — it makes it scientifically interesting, which is a different thing entirely.
Why People Use It
Despite having no FDA-approved medical indication, an estimated 1 to 15 million Americans use kratom regularly, according to various survey estimates. They’re reaching for it for a cluster of overlapping reasons:
Pain management is the most commonly cited use. Many users are chronic pain patients who feel underserved by conventional medicine, particularly in the context of prescription opioid restrictions following the opioid crisis. For them, kratom fills a gap — imperfectly and unofficially.
Recreational effects and euphoria are also part of the picture, particularly at higher doses. At lower doses, kratom tends to produce stimulant-like effects: increased alertness and energy. At higher doses, it shifts toward sedation and euphoria, more typical of opioid-class substances.
Anxiety and stress relief round out the picture. Many users describe kratom as calming without the cognitive fog associated with benzodiazepines, making it appealing for stress management.
Safety Profile and the Research Gap
Here’s the honest assessment: the safety profile of kratom is poorly characterized. Clinical research is sparse, long-term human data is limited, and most of what we know comes from case reports, surveys, and animal studies. The FDA has attributed a number of deaths to kratom, though critics note that most of these cases involved polydrug use, making causation difficult to establish.
Known risks include nausea, liver toxicity (in rare cases), dependence, and withdrawal symptoms. The absence of robust clinical trials means neither a full harm profile nor a clear therapeutic window has been established.
The DEA’s Attempted Scheduling — and a Remarkable Public Pushback
In August 2016, the DEA made an extraordinary announcement: it planned to place kratom’s primary alkaloids into Schedule I of the Controlled Substances Act — the most restrictive category, reserved for drugs with “no accepted medical use” and “high abuse potential,” alongside heroin and LSD. The agency invoked its emergency scheduling authority, intending to bypass the usual public comment process.
The public response was swift and organized. Tens of thousands of citizens submitted comments. Patients, researchers, and advocacy groups flooded congressional offices with calls and letters. A bipartisan group of 51 members of Congress signed a letter asking the DEA to withdraw the emergency scheduling action and allow for scientific review. The American Kratom Association organized nationally.
In an unusual reversal, the DEA withdrew its intent to emergency schedule kratom in October 2016, citing the unprecedented public response and agreeing to an open comment period. The FDA has since issued warnings and pursued enforcement actions against kratom products, but as of this writing, kratom remains legal at the federal level although several states have banned it individually.
This episode is a compelling case study in civic engagement. A well-informed, organized public, armed with scientific arguments and personal testimony, reversed a major regulatory agency’s plans. Whatever your views on kratom, the policy episode is a reminder that public participation in regulatory processes is not theater; it can actually work.
Dependency, Addiction, and the Opioid Withdrawal Question
Kratom’s partial agonist activity at mu-opioid receptors means it does carry dependence and addiction potential. Regular users can develop tolerance and experience withdrawal symptoms upon cessation, including muscle aches, insomnia, irritability, and anxiety. These symptoms resemble, though are generally considered milder than, classic opioid withdrawal.
Perhaps most intriguingly, kratom is used by some individuals as a self-managed tool for opioid withdrawal and harm reduction essentially stepping down from more potent opioids using kratom as a bridge. Anecdotal reports describe meaningful symptom relief. However, this practice has not been validated in clinical trials, carries its own dependency risks, and is not endorsed by medical authorities. Replacing one opioid-acting substance with another is a strategy that requires careful medical supervision, not a DIY solution.
The Bottom Line
Kratom sits in a genuinely complicated space — scientifically fascinating, pharmacologically plausible in some of its claimed mechanisms, politically volatile, and practically under-studied. Its G-protein biased mechanism of action is legitimately interesting to researchers. Its role in the lives of pain patients is real and often deeply felt. Its risks are real and not fully mapped. And its near-scheduling and subsequent reversal is a rare, instructive example of democratic engagement shaping drug policy.
If you’re a patient, a biohacker, or simply someone curious about the frontier where ethnobotany meets neuropharmacology, kratom deserves your critical attention — not uncritical enthusiasm, and not reflexive dismissal. What it deserves most, frankly, is the rigorous clinical research that has so far been lacking. Until that exists, the conversation will remain exactly where it is: fascinating, unresolved, and urgently worth having.
This article is for informational purposes only and does not constitute medical advice. If you are managing pain, opioid use disorder, or considering kratom, consult a qualified healthcare provider.
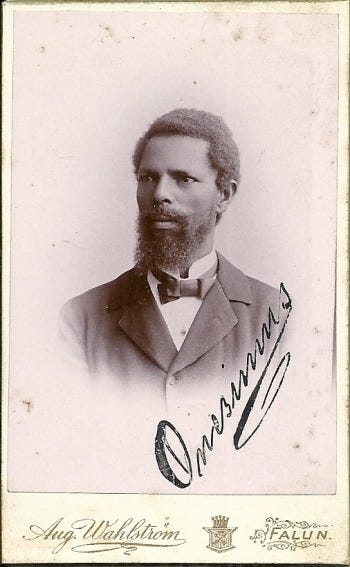
Long before Edward Jenner administered his famous cowpox vaccine in 1796, long before the word “vaccination” even existed, a man whose freedom had been stolen brought a life-saving idea across an ocean. His name was Onesimus, and his knowledge may have saved thousands of lives in colonial Boston, yet history nearly forgot him entirely.
A Man, Not a Name
Around 1706, the Puritan minister Cotton Mather received an enslaved African man as a gift from his congregation in Boston, Massachusetts. Mather gave him the name Onesimus, after the enslaved person in Paul’s letter to Philemon in the New Testament — an irony that likely was not lost on the man who bore it. We know almost nothing about Onesimus’s origins, his family, or the circumstances of his capture and transport. He existed in the historical record largely as property.
But Onesimus carried something with him that no one could enslave: knowledge.
An Old Practice from Distant Lands
When Mather questioned Onesimus about smallpox — a disease that was devastating colonial populations — the man described a practice he had known in Africa. He had been deliberately inoculated as a child, explaining that material from the pustules of a smallpox sufferer had been introduced into a cut in his skin. The procedure, he told Mather, had given him a mild illness that left him immune to the disease afterward. He showed Mather the scar on his arm as evidence.
Mather was fascinated. What Onesimus described was the practice of variolation, purposeful infection with material from smallpox lesions to provoke a controlled, usually milder version of the disease and confer lasting immunity. The practice had been known for centuries in parts of Africa, the Ottoman Empire, and China. In 1714 and 1716, Mather also read letters in the Philosophical Transactions of the Royal Society from physicians in Constantinople describing the same technique. But it was Onesimus who made it immediate, personal, and urgent for him.
Boston’s Deadly Epidemic
The moment of truth came in 1721, when a British warship carried smallpox into Boston Harbor. The disease tore through a city of about 11,000 people. By the end of the epidemic, nearly half the population had been infected and roughly 850 had died. It was one of the deadliest outbreaks in American colonial history.
Mather, armed with the knowledge Onesimus had given him and the corroborating accounts from the Royal Society, lobbied Boston’s physicians to attempt inoculation on a wide scale. He was met with fierce resistance. Most doctors were skeptical or outright hostile, and the public was alarmed with many believing that deliberately introducing the disease was reckless or even blasphemous. An angry Bostonian threw a crude bomb through Mather’s window with a note condemning the practice.
Only one physician, Dr. Zabdiel Boylston, agreed to try. Boylston inoculated 242 people during the epidemic. Of those, just six died, a mortality rate of about 2 percent, compared to roughly 15 percent among those who contracted the disease naturally. The numbers made a compelling case that couldn’t be ignored.
The Legacy Stolen and Reclaimed
Edward Jenner’s 1796 discovery that cowpox inoculation could prevent smallpox was genuinely revolutionary, safer, more reproducible, and the true foundation of modern immunology. History rightly honors him. But the concept of deliberately inducing immunity predated Jenner by generations, and its introduction to the English-speaking world traveled through the mind and memory of an enslaved African man in Boston.
Edward Jenner English Physician, “Father of Immunology”
Onesimus was eventually able to purchase a partial measure of his freedom from Mather by finding a replacement enslaved person, a transaction that reminds us how brutal the system was that surrounded his remarkable contribution.
His name deserves to be remembered not as a footnote, but as a pioneer. The idea that a community could be defended from disease by confronting it deliberately, that immunity could be manufactured, is one of the most powerful ideas in the history of medicine. And in America, it began with Onesimus.
There are bodybuilders who win titles, and then there are bodybuilders who change the entire conversation about what it means to train. Mike Mentzer was emphatically the latter. Born on November 15, 1951, in the Germantown section of Philadelphia and raised in Ephrata, Pennsylvania, Mentzer was never just a guy who lifted weights. He was a contrarian philosopher, a pre-med dropout, an Air Force veteran, and ultimately a tragic figure whose legacy burns brighter today than it did the day he died.
The Kid from Ephrata
Mentzer came from a working-class family of German-Italian heritage. His father, Harry, was not an intellectual but deeply valued knowledge and rewarded academic performance — cash for good grades, a baseball mitt for effort. Mike internalized that equation early. He was a straight-A student through grammar school and Ephrata High School, later crediting his English teacher Elizabeth Schaub for his love of language and analytical thinking.
At age 12, after spotting a photo of Steve Reeves on the cover of Muscle Builder/Power magazine, Mentzer asked for a barbell set for Christmas. He got one. By 15, he was bench pressing 370 pounds at a bodyweight of 165 lbs, numbers that would make grown men question their existence. He attended the very first Mr. Olympia contest in 1965 and later described it as “almost a religious experience.”
After high school, he enlisted in the United States Air Force, where he trained six days a week, two-plus hours a day, the conventional approach he would later dismantle entirely. He simultaneously enrolled at the University of Maryland as a pre-med student, studying genetics, physical chemistry, and organic chemistry, before bodybuilding pulled him away from the psychiatrist’s chair he’d been aiming for.
The Titles: A Perfect Record
Mentzer didn’t just win competitions; he dominated them with mathematical precision.
After a serious shoulder injury shelved him from 1971 to 1974, he came back leaner, meaner, and philosophically sharpened. In 1976, he won the Mr. America title. In 1977, he won the North American Championships. Then in 1978, at the Mr. Universe in Acapulco, Mexico, Mentzer achieved something no one had done before or has done since: he posted a perfect score of 300, flawless across every judge, every category. He turned pro on the spot.
In 1979, he won the heavyweight division at the Mr. Olympia, again with a perfect score. The man was doing things that shouldn’t have been possible.
The Arnold Conflict: The Wound That Never Healed
Then came 1980. The Sydney Mr. Olympia. And the most controversial result in the history of professional bodybuilding.
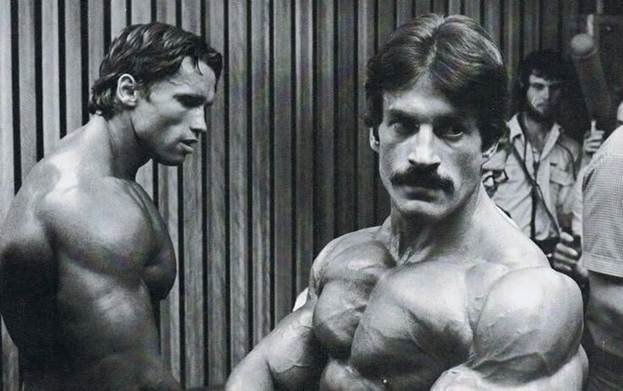
Arnold Schwarzenegger, who had been semi-retired pursuing his acting career, made a surprise comeback. The consensus among athletes, journalists, and fans on the ground was that Arnold was not in peak condition, certainly not Olympia-winning condition. Yet Arnold took first. Mentzer placed fourth, tied with Boyer Coe, behind Schwarzenegger, Chris Dickerson, and Frank Zane.
Arnold and Mike, Sydney
Mentzer never claimed he should have won. What he claimed, loudly and repeatedly until the day he died, was that Arnold shouldn’t have. He believed the result was predetermined, a political decision by the Weider empire to protect its most bankable name. The contest broke something in him. He retired from competition at 29, a decision that robbed the sport of what should have been his dominant decade.
In the years that followed, Mentzer’s comments about Schwarzenegger were scorched-earth. Arnold, for his part, eventually reached out, and the two reportedly reconciled by phone before Mentzer’s death. But the wound never fully closed. For Mentzer, the 1980 Olympia wasn’t just a loss; it was evidence that rationality and merit had no place in the sport he’d given his life to.
The Downward Spiral: Drugs, Isolation, and Decline
After 1980, Mentzer’s personal life unraveled in spectacular and heartbreaking fashion. He descended into a period of heavy drug use, including amphetamines, initially justified as productivity aids during contest prep, but which escalated well beyond that. He also battled severe depression, exacerbated by his disenfranchisement from the sport and his growing sense that the bodybuilding establishment had stolen something from him that could never be returned.
He became increasingly isolated, obsessive, and volatile. He withdrew from the public eye for much of the 1980s. His personal relationships suffered. He was hospitalized for heart problems in his later years and put on blood thinners and painkillers. By the time he began reclaiming his public voice through Iron Man magazine in the late ’80s and early ’90s, mentoring athletes like Dorian Yates (who credited Mentzer’s Heavy Duty principles for his six Mr. Olympia wins), the man coaching others looked nothing like the golden statue of 1978.
On June 10, 2001, Mike Mentzer died of heart complications at age 49. His younger brother Ray Mentzer, himself a Mr. America winner in 1979, discovered the body. Ray, who had been battling a rare and debilitating kidney disorder, died within 48 hours of his brother. The bodybuilding world lost two Mentzers in two days.
The Heavy Duty Revolution: Less Is Shockingly More
Here’s where things get genuinely fascinating for anyone who trains, experiments with peptides, or thinks seriously about the biology of hypertrophy.
While every elite bodybuilder of Mentzer’s era was grinding through marathon sessions — two to three hours a day, six days a week, 20-plus sets per muscle group — Mentzer was going to war for 45 minutes every four to seven days. Fewer than five working sets per session. Exercises taken to absolute muscular failure, then employing forced reps, negative reps, and static holds to push beyond the edge of the possible.
His contemporaries — Arnold, Robby Robinson, Lou Ferrigno — believed volume was the variable that mattered most. Mentzer, drawing heavily on Arthur Jones’s earlier high-intensity work and grounding it in stress physiology, argued the opposite: intensity is the stimulus; rest is where growth actually happens. Overtraining wasn’t a risk, in his view — it was what almost everyone was doing, all the time.
The results on his own body were undeniable. He was carrying 225–235 lbs of competition-ready muscle at 5’8″, achieving perfect scores in sanctioned IFBB competition, training fewer hours per week than most recreational gym-goers. Something was clearly working.
The Myostatin Theory: Was Mentzer Genetically Hacked Before Anyone Knew It Was Possible?
This is the question that keeps biohackers and peptide researchers up at night.
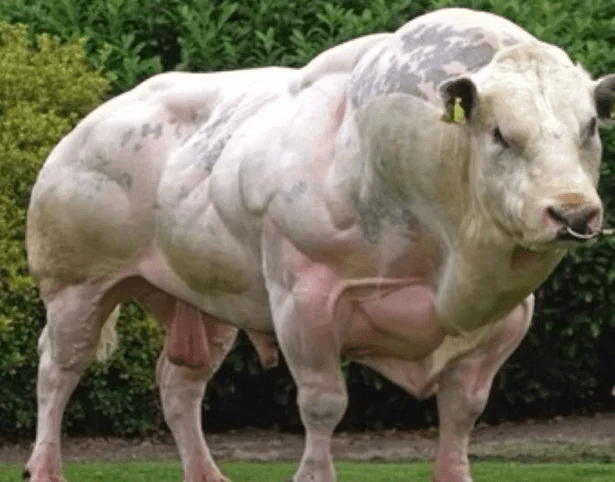
Myostatin is a protein encoded by the MSTN gene that functions as a brake on muscle growth. It tells your body: enough muscle, stop building. In animal models — Belgian Blue cattle, whippet dogs, and in rare human cases — loss-of-function mutations in the myostatin gene produce individuals with dramatically elevated muscle mass, lower body fat, and extraordinary strength, often from early childhood.
Belgian Blue Bull
Here’s what makes Mentzer’s case intriguing: the sheer efficiency of his development doesn’t map cleanly onto even the most optimized conventional training and pharmacological protocols. He was gaining and maintaining freakish muscle mass on training volumes that mainstream science says should have been inadequate. He responded to intensity in ways his peers simply didn’t. He could afford rest periods his contemporaries would have called career suicide.
A partial loss-of-function mutation in MSTN — not a complete knockout, but a reduced-function variant — could explain this. Such a mutation would lower the myostatin “ceiling,” allowing greater hypertrophic response to each training stimulus, faster recovery, and a lower threshold for achieving maximal development. You wouldn’t need to accumulate 20 sets of volume to hit the growth trigger — a handful of brutally intense sets might fully saturate the pathway.
This is speculative; Mentzer was never genetically tested for this. But the hypothesis is coherent and consistent with the observed data. Combine a potential myostatin variant with intelligent steroid use (he was open about using anabolics, as was universal in the sport), and you have a biological profile that could genuinely thrive on the Heavy Duty system while peers using identical protocols would overtrain and plateau.
The Legacy: Ahead of His Time, Behind Enemy Lines
Mike Mentzer was right about a lot of things that took the fitness world decades to catch up on — the primacy of intensity over volume, the critical role of recovery, the individualization of training stimuli. Modern high-intensity training, rest-pause protocols, and even the growing mainstream interest in myostatin inhibitors as a therapeutic target all carry Mentzer’s fingerprints, whether or not his name is attached.
He was also deeply flawed — consumed by bitterness, derailed by substances, unable to separate his philosophical certainty from his personal grievances. He burned bridges, alienated allies, and spent years in a fog when he could have been building.
But the physique was real. The perfect score was real. The philosophy was internally consistent and scientifically grounded in ways his critics rarely acknowledged.
Mike Mentzer didn’t just train differently. He trained as if he knew something the rest of the field didn’t — about the body, about intensity, and perhaps, about his own unusual biology. Whether that knowledge was earned through intellect, granted by genetics, or both, the results spoke for themselves on every stage he stood on.
The tragedy isn’t that he died at 49. The tragedy is that he stopped competing at 29.
A daughter of Harvard, a pioneer of microbiology, and a barrier-breaking veterinarian — Jane Hinton’s life story is one of quiet brilliance and enduring impact.
Roots of Greatness: Early Life and Family
Jane Hinton was born on May 1, 1919, in Canton, Massachusetts, into a household where intellectual excellence was simply the family tradition. Her mother, Ada (Hawes) Hinton, was a former teacher and social worker, and her father, William Augustus Hinton, was one of the most distinguished African American scientists of the twentieth century. Growing up in such an environment, it was all but inevitable that Jane would carve her own remarkable path through the sciences.
Education was a serious priority in the Hinton household and not without reason. Knowing that racial barriers in the United States could limit their daughters’ opportunities, William and Ada made the bold decision to send Jane and her sister to school across several countries in Europe when Jane was just six years old. The girls received a broad, rigorous education abroad before returning to the United States in 1928. Jane completed her secondary education at Montpelier Seminary in Vermont, graduating in 1935, and went on to earn her bachelor’s degree from Simmons College in Boston in 1939.
Her Father’s Shadow and Legacy
To understand Jane Hinton, you must first understand her father. William Augustus Hinton (1883–1959) was a bacteriologist and pathologist whose parents had been enslaved, a fact that makes his achievements all the more extraordinary. Faced with widespread racism in Boston’s medical establishment, he channeled his ambitions into laboratory medicine and rose to become one of the field’s foremost authorities. In the 1920s, he developed the “Hinton Test,” a blood serology test for syphilis that was widely used across the United States until more advanced methods superseded it after World War II.
William Augustus Hinton
William Hinton’s firsts were staggering: he became the first African American to teach at Harvard Medical School and the first African American author to publish a medical textbook. In 1931, he also created a course on medical laboratory techniques that was notably open to women, a forward-thinking move that helped shape the next generation of laboratory scientists, including his own daughter. Jane would go on to work directly in her father’s Harvard laboratory after college, where a world-changing discovery awaited her.
The Mueller-Hinton Agar: A Tool That Transformed Medicine
After graduating from Simmons College, Jane joined Harvard University’s Department of Bacteriology and Immunology as an assistant to microbiologist Dr. John Howard Mueller. Together, in 1941, they published a landmark paper and introduced what would become one of the most essential tools in modern microbiology: the Mueller-Hinton agar.
So what exactly is it? Agar is a gel-like medium derived from seaweed used in laboratories to grow and study microorganisms. The Mueller-Hinton agar is a specially formulated version designed to cultivate a wide range of bacteria in a non-selective, non-differential environment, meaning it encourages the growth of many species without distinguishing between them. Mueller and Hinton discovered that incorporating starch into the agar served a critical dual purpose: it boosted bacterial growth while simultaneously absorbing bacterial toxins that would otherwise interfere with antibiotic testing. This made the medium remarkably clean and reliable.
Originally developed to isolate Neisseria bacteria, the pathogens responsible for meningococcal meningitis and gonorrhea, the Mueller-Hinton agar proved far more versatile than its creators may have anticipated. Its loose, permeable consistency allows antibiotics to diffuse evenly through the medium, which turned out to be ideal for antibiotic susceptibility testing. By the 1960s, it had become the go-to substrate for the Kirby-Bauer disk diffusion method, a test in which antibiotic-saturated paper disks are placed on a bacteria-covered plate to determine whether a drug can inhibit bacterial growth. The Clinical and Laboratory Standards Institute ultimately adopted the Kirby-Bauer technique on Mueller-Hinton agar as the global gold standard for antibiotic resistance testing, a designation it still holds today.
In an era when antibiotic resistance threatens to undo decades of medical progress, the Mueller-Hinton agar is more relevant than ever. Laboratories worldwide still reach for this medium whenever they need to know whether a bacterium can be stopped by a given antibiotic, a question at the very heart of treating infections.
War, Veterinary Medicine, and Another Barrier Broken
When World War II erupted, Jane Hinton took her skills directly into the war effort. From 1942 to 1945, she worked as a medical technician with the U.S. War Department in Arizona, serving in the laboratory of Dr. Hildrus Augustus Poindexter, whose team’s work combating malaria and tropical diseases in the Pacific earned Poindexter a Bronze Star. Hinton’s own contributions to this critical public health work, though less formally decorated, were no less real.
After the war, Hinton charted a new course. She enrolled in the School of Veterinary Medicine at the University of Pennsylvania, a daunting environment in which fewer than five African Americans had ever graduated before her. She threw herself into student life, serving as both class historian and class secretary, and earned her Doctor of Veterinary Medicine (VMD) in 1949. That same year, Alfreda Johnson Webb earned her VMD from Tuskegee University. The two women made history together as the first African American women to become doctors of veterinary medicine in the United States, and the first African American members of the Women’s Veterinary Medicine Association.
A Life Well Lived: Career, Legacy, and Quiet Retirement
Returning to her hometown of Canton, Massachusetts, Hinton practiced as a small animal veterinarian until 1955, before transitioning to a role as a federal government inspector with the U.S. Department of Agriculture in Framingham, where she focused on researching and responding to disease outbreaks in livestock. She retired around 1960, at just 41 years old, and spent her later years tending a garden and caring for an assortment of pets. She never married. Jane Hinton passed away on April 9, 2003, just weeks before what would have been her 84th birthday.
In 1984, the Minority Veterinary Students association at the University of Pennsylvania honored Hinton alongside John Taylor, the first African American graduate of the school’s veterinary program during the school’s centennial celebrations. It was a recognition long overdue.
Jane Hinton never sought the spotlight. Yet in two entirely different fields — microbiology and veterinary medicine — she left marks that have never faded. Every hospital laboratory that runs an antibiotic sensitivity test today is building on the work she did at Harvard more than eighty years ago. And every Black woman who enters veterinary school walks a path that Hinton helped pave.
In the mid-1990s, a breakthrough in obesity research fundamentally changed our understanding of how the body regulates weight, hunger, and metabolism. The discovery of leptin, a hormone that would prove central to energy balance, emerged from decades of research involving an unusual laboratory mouse strain and culminated in findings that would help patients with rare but devastating metabolic disorders. This is the story of how scientific curiosity, persistence, and a colony of obese mice led to one of the most significant discoveries in modern endocrinology.
The Mystery of the OB Mouse
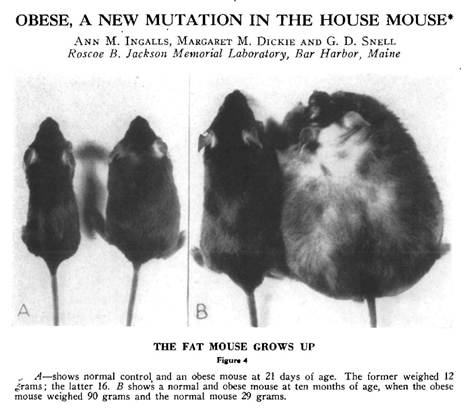
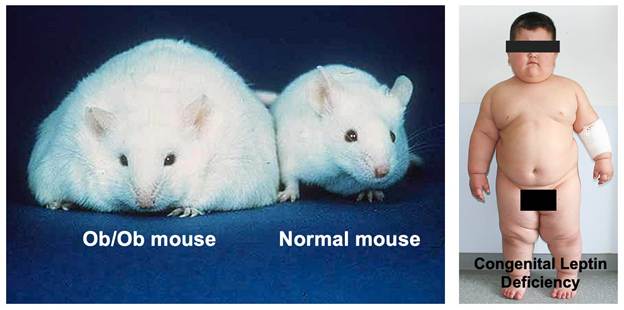
The story begins in 1949 at the Jackson Laboratory in Bar Harbor, Maine, where researchers noticed something extraordinary: a spontaneous mutation had produced mice that became massively obese. These mice, which came to be known as the “ob/ob” mice (short for “obese”), weighed nearly three times as much as their normal littermates. They were voraciously hungry, ate constantly, and developed severe obesity along with diabetes-like symptoms.
For decades, these ob/ob mice remained a biological curiosity. Scientists knew the obesity was caused by a recessive genetic mutation, meaning both copies of a particular gene had to be defective for the condition to appear, but the identity and function of that gene remained elusive. The mice became an invaluable research tool, but the fundamental question persisted: what was different about these animals at the molecular level?
Adding to the intrigue was the existence of another mutant mouse strain called “db/db” (for “diabetes”), discovered in the 1960s. These mice had a remarkably similar phenotype to the ob/ob mice—they too were obese, constantly hungry, and diabetic. Yet they had a different genetic mutation. The relationship between these two strains would prove crucial to understanding the biology of weight regulation.
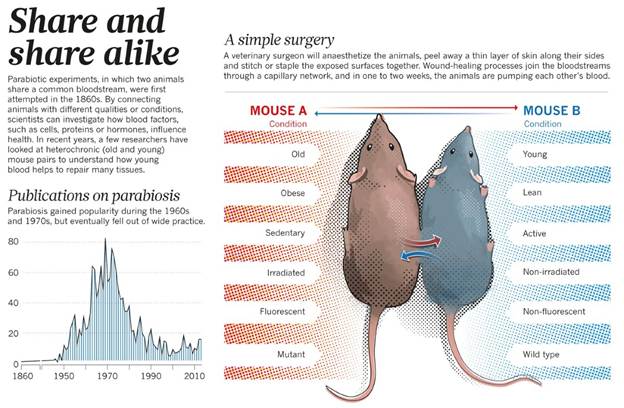
Parabiosis: A Clue from Connected Mice
A pivotal insight came from elegant experiments conducted in the 1970s by Douglas Coleman at the Jackson Laboratory. Coleman performed parabiosis experiments—surgically joining two mice so they shared a circulatory system. When he connected an ob/ob mouse to a normal mouse, something remarkable happened: the obese mouse ate less and lost weight. However, when he connected a db/db mouse to a normal mouse, the normal mouse stopped eating and became emaciated, while the db/db mouse remained obese.
These results suggested a powerful hypothesis: the ob/ob mice lacked some circulating factor that suppressed appetite and promoted energy expenditure, while the db/db mice produced this factor but couldn’t respond to it. In other words, ob mice couldn’t make the signal, while db mice couldn’t receive it. The circulating factor was being produced by the normal mouse and affecting the ob mouse through their shared bloodstream, but the db mouse appeared to be overproducing the factor to no effect, overwhelming its normal partner.
Coleman’s work provided a conceptual framework, but identifying the actual molecule would require tools that didn’t yet exist. The answer would have to wait for the molecular biology revolution.
Jeffrey Friedman and the Hunt for the OB Gene
Enter Dr. Jeffrey Friedman, a physician-scientist at Rockefeller University who became fascinated with understanding the genetic basis of obesity. In the late 1980s, Friedman set out to identify and clone the ob gene using an approach called positional cloning, a painstaking technique that involves tracking down a gene based solely on its chromosomal location without any prior knowledge of what the gene does or what protein it produces.
This was an audacious undertaking. The mouse genome had not been sequenced. The techniques for positional cloning were still being developed. The project would require mapping the mutation to a specific chromosomal region, narrowing down that region through genetic linkage analysis, identifying candidate genes, and then proving which one was responsible for the obesity phenotype.
Friedman’s laboratory spent years on this pursuit. Using genetic markers and analyzing thousands of mice from breeding crosses between ob/ob mice and normal mice, they progressively narrowed down the location of the ob gene on mouse chromosome 6. They eventually identified a region containing only a handful of genes. The team then systematically examined each candidate gene, looking for differences between normal mice and ob/ob mice.
The breakthrough came in 1994. After nearly eight years of intensive research, Friedman’s team identified the ob gene. The gene coded for a previously unknown protein that was expressed primarily in white adipose tissue—body fat. In ob/ob mice, the gene contained a mutation that prevented production of functional protein. The team named the protein “leptin,” derived from the Greek word “leptos,” meaning thin.
The Science Behind the Discovery
The identification of leptin represented a triumph of molecular biology techniques. Friedman’s team used several key approaches:
Genetic Mapping: By breeding ob/ob mice with normal mice from different strains, researchers could track which genetic markers co-segregated with the obesity phenotype across generations. This allowed them to progressively narrow the chromosomal region containing the ob gene from millions of base pairs down to a manageable segment.
Physical Mapping: Once the region was identified, the team created overlapping clones of DNA fragments covering that area—a technique called “chromosome walking.” This allowed them to systematically examine the DNA sequence of the candidate region.
Candidate Gene Analysis: Within the narrowed region, researchers looked for sequences that resembled known genes. They identified several candidates and examined their expression patterns and sequence variations between normal and obese mice.
Mutation Analysis: The crucial evidence came when they found that ob/ob mice had a mutation in one particular gene that caused a premature stop signal in the protein-coding sequence. This meant the gene couldn’t produce a functional protein. A different natural mutation in another strain of obese mice affected the same gene differently but with the same result—no functional leptin.
Expression Studies: The researchers demonstrated that the ob gene was expressed primarily in adipocytes (fat cells) and that the level of expression correlated with the amount of body fat. They showed that normal mice produced leptin in proportion to their fat stores, while ob/ob mice produced none.
The final proof came from administering leptin to ob/ob mice. When given injections of the leptin protein, these previously insatiable, obese mice ate less, became more active, and lost weight dramatically. Their metabolism normalized. It was a stunning validation of decades of hypothesis and years of painstaking molecular work.
What Does Leptin Do?
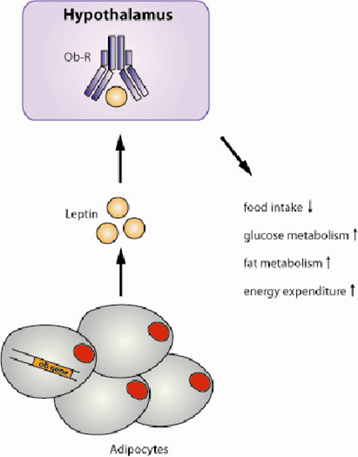
The discovery of leptin revealed a sophisticated system for regulating body weight and energy balance. Leptin functions as an adiposity signal, essentially, fat tissue uses leptin to communicate with the brain about the body’s energy stores.
Here’s how the system works: adipocytes produce leptin in proportion to the amount of fat they contain. More body fat means more leptin production. The leptin circulates in the bloodstream and travels to the brain, where it binds to receptors concentrated in the hypothalamus, a region critical for regulating appetite, metabolism, and energy expenditure.
When leptin levels are adequate, the brain receives the signal that energy stores are sufficient. This triggers several responses: appetite decreases, energy expenditure increases through mechanisms like thermogenesis (heat production), and the body shifts toward using stored energy. The hypothalamus also regulates other hormones and physiological processes to maintain energy balance.
Conversely, when leptin levels drop—as happens during weight loss or starvation—the brain interprets this as a signal that energy stores are depleted. Hunger increases, metabolism slows to conserve energy, and the body shifts toward storing any available calories as fat. This is why losing weight becomes progressively harder—the body fights to defend its fat stores through leptin-mediated mechanisms.
The db/db mice, it turned out, had mutations in the leptin receptor gene. They produced leptin, often at very high levels, but their brains couldn’t respond to it. This explained Coleman’s parabiosis results: the circulating leptin from db mice entered the normal mice and suppressed their appetite, while the db mice themselves remained obese because they couldn’t sense the hormone.
From Mice to Humans: The Leptin Connection
Friedman’s discovery immediately raised a critical question: was leptin relevant to human obesity? The answer proved complex. In 1997, researchers identified the first humans with congenital leptin deficiency, children from consanguineous families who, like ob/ob mice, had mutations in both copies of their leptin gene.
These children presented with a dramatic phenotype: they were born at normal weight but rapidly developed severe obesity in early childhood, often reaching extreme weights by age 5 or 6. They had insatiable hunger, constantly seeking food, and displayed food-seeking behaviors that disrupted family life. They also had delayed puberty due to hypogonadotropic hypogonadism, leptin’s absence prevented normal sexual maturation.
The medical implications extended beyond obesity. Many patients with congenital leptin deficiency developed severe metabolic complications:
Lipodystrophy-like Features: While the genetic form involves too little leptin from too much fat, patients with lipodystrophy, a group of disorders characterized by loss of body fat, also have leptin deficiency, but from the opposite cause: too little fat tissue. Whether from genetic mutations or acquired fat loss, the lack of leptin causes similar metabolic derangements.
Severe Hypertriglyceridemia: Leptin deficiency causes marked elevations in triglycerides, sometimes reaching levels over 1000 mg/dL or higher. This creates visible lipemia—the blood plasma appears milky white due to excess fat particles. Such extreme elevations dramatically increase the risk of pancreatitis, a potentially life-threatening inflammation of the pancreas.
Fatty Liver Disease: Without adequate leptin signaling, the liver accumulates excessive fat, leading to hepatic steatosis and potentially progressing to more severe liver damage.
Insulin Resistance and Diabetes: The metabolic dysfunction extends to glucose metabolism, with many leptin-deficient patients developing insulin resistance and type 2 diabetes at young ages.
Immune Dysfunction: Leptin plays a role in immune function, and deficient patients often have increased susceptibility to infections.
Leptin Replacement: A Remarkable Treatment
When leptin-deficient patients were identified, the obvious treatment approach was leptin replacement therapy—essentially, providing the hormone these patients couldn’t make. The results were nothing short of miraculous.
Children and adults with congenital leptin deficiency who received recombinant leptin (metreleptin) experienced dramatic transformations. Within weeks to months of starting treatment, patients showed:
Marked Weight Loss: Patients lost substantial weight, sometimes 50% or more of their body weight over the first year of treatment. The weight loss continued until they reached near-normal weight ranges.
Normalized Eating Behavior: The constant hunger disappeared. Patients who had been consumed by food-seeking behavior developed normal appetite regulation. Families reported life-changing improvements in quality of life.
Resolution of Metabolic Abnormalities: Triglyceride levels plummeted from dangerous elevations to normal ranges within weeks. The lipemia resolved. Fatty liver improved. Glucose metabolism normalized.
Sexual Development: Children with delayed puberty began normal pubertal progression. Adults with hypogonadism experienced normalization of sex hormones.
Improved Quality of Life: Beyond the physical changes, patients reported profound improvements in well-being, energy, and ability to participate in normal activities.
The treatment was equally effective in patients with acquired lipodystrophy. Whether from genetic causes, autoimmune destruction of fat tissue, or HIV treatment-related fat loss, patients with severe lipodystrophy and leptin deficiency showed similar dramatic responses to leptin replacement. The FDA approved metreleptin in 2014 specifically for treating complications of leptin deficiency in patients with congenital or acquired lipodystrophy.
The Broader Impact and Unexpected Discoveries
The leptin story illustrates both the power and the limitations of translational research. While leptin replacement is spectacularly effective for the rare patients with leptin deficiency, it largely failed as a treatment for common obesity. Most obese people have high leptin levels—their problem isn’t leptin deficiency but leptin resistance, where the brain fails to respond appropriately to the hormone’s signal. This parallels type 2 diabetes, where the problem is usually insulin resistance rather than insulin deficiency.
Nevertheless, leptin research opened entire new fields of investigation. Scientists discovered that leptin is part of a complex network of hormones and neural circuits regulating energy balance. The hypothalamic pathways that respond to leptin have been mapped in extraordinary detail. We now understand that leptin regulates not just appetite and metabolism but also immunity, reproduction, bone metabolism, and many other physiological systems.
The discovery validated the concept that body weight is biologically regulated—that the body has sophisticated mechanisms for sensing and defending its energy stores. This shifted the conversation about obesity from one of simple willpower to recognition of underlying biological drives that make weight loss and maintenance challenging.
Legacy of Discovery
Jeffrey Friedman’s identification of leptin stands as one of the landmark achievements in metabolism research. The work earned him numerous awards, including the Lasker Award (often called “America’s Nobel”) and the Shaw Prize. More importantly, it provided:
Understanding of Weight Regulation: Leptin revealed that body weight isn’t simply a matter of calories in versus calories out, but involves active biological regulation through hormonal signaling between fat tissue and the brain.
Treatment for Rare Diseases: For patients with congenital leptin deficiency or lipodystrophy, leptin replacement is genuinely life-saving, preventing deadly complications like pancreatitis and providing normal quality of life.
Research Framework: The discovery established paradigms for studying energy homeostasis and identified key neural circuits in the hypothalamus that have become targets for developing new metabolic therapies.
Validation of Genetic Approaches: The success of positional cloning to identify leptin validated this approach and paved the way for identifying many other disease genes.
The story of leptin demonstrates how basic research—studying mutant mice in a laboratory—can lead to profound clinical applications. Those ob/ob mice that puzzled researchers in 1949 eventually revealed fundamental truths about how our bodies regulate weight and led to treatments that transformed lives for patients with devastating metabolic disorders.
The journey from a curious mutation in mice to a life-saving treatment for humans took nearly half a century. It required insights from genetics, molecular biology, endocrinology, and clinical medicine. It stands as a testament to the value of basic research and the unexpected ways that understanding fundamental biology can ultimately benefit human health. The ob mouse, once just an oddity in a research colony, became the key to unlocking one of metabolism’s most important secrets.
When most people think of Viagra (sildenafil) or Cialis (tadalafil), they associate these medications exclusively with male sexual dysfunction. However, researchers have long been curious about whether these drugs might offer similar benefits for women experiencing sexual difficulties. The answer, as it turns out, is considerably more complex than a simple yes or no.
Understanding the Pharmacology: How PDE5 Inhibitors Work
To understand whether these medications could help women, we first need to explore how they work at the biochemical level.
The Nitric Oxide Pathway
Both Viagra and Cialis belong to a class of drugs called phosphodiesterase type 5 (PDE5) inhibitors. Their mechanism of action centers on the nitric oxide (NO) signaling pathway, which plays a crucial role in smooth muscle relaxation throughout the body.
Here’s how the cascade works:
Step 1: Sexual Stimulation and Nitric Oxide Release When sexual arousal occurs (through physical or psychological stimulation), nerve endings and endothelial cells lining blood vessels release nitric oxide. This is a critical first step that these medications cannot replace or initiate on their own.
Step 2: Activation of Guanylate Cyclase Nitric oxide binds to and activates an enzyme called guanylate cyclase within smooth muscle cells. This enzyme then converts guanosine triphosphate (GTP) into cyclic guanosine monophosphate (cGMP).
Step 3: cGMP and Smooth Muscle Relaxation The accumulation of cGMP triggers a series of events that ultimately lower calcium levels within smooth muscle cells. This reduction in intracellular calcium causes the smooth muscles surrounding blood vessels to relax, leading to vasodilation (widening of blood vessels) and increased blood flow to the tissue.
Step 4: The Role of PDE5 Under normal circumstances, an enzyme called phosphodiesterase type 5 (PDE5) breaks down cGMP, which eventually returns the smooth muscle to its non-relaxed state and reduces blood flow back to baseline levels.
Step 5: How PDE5 Inhibitors Work Viagra and Cialis work by selectively inhibiting PDE5, preventing it from breaking down cGMP. This allows cGMP to accumulate to higher levels and persist for longer periods, prolonging smooth muscle relaxation and maintaining increased blood flow to the target tissues.
Key Biochemical Principle
It’s essential to understand that PDE5 inhibitors do not create arousal or initiate the nitric oxide cascade. They simply amplify and prolong the body’s natural response to sexual stimulation by preventing the breakdown of cGMP. Without the initial release of nitric oxide from arousal, these medications have little to no effect.
Effects on Muscles and Blood Flow
The smooth muscle relaxation induced by PDE5 inhibitors affects blood vessels throughout the body, though the medications show some tissue selectivity.
In Men
In men, PDE5 is highly concentrated in the corpus cavernosum of the penis. When PDE5 is inhibited, blood flow to this erectile tissue increases dramatically, facilitating and maintaining an erection sufficient for sexual activity. The mechanism is straightforward: increased blood flow leads to engorgement, which produces the physical changes necessary for penetrative intercourse.
In Women: The Anatomical Parallel
Women have analogous erectile tissues that respond to increased blood flow during arousal:
Clitoral tissue: The clitoris contains erectile tissue that engorges with blood during arousal, similar to penile tissue
Vaginal walls: Increased blood flow leads to vaginal lubrication through transudate (fluid passing through vessel walls)
Labia: The labia minora and majora also experience increased blood flow and engorgement during arousal
Theoretically, PDE5 inhibitors should enhance blood flow to these tissues in women just as they do in men, since the underlying biochemical mechanisms are identical. Studies have confirmed that these medications do indeed increase genital blood flow in women.
The Critical Question: Does Increased Blood Flow Equal Enhanced Sexual Function?
This is where the science becomes fascinating and reveals a fundamental difference between male and female sexual response.
What the Research Shows
Multiple clinical trials have investigated whether Viagra or Cialis improve sexual function in women, particularly those with sexual arousal disorder or hypoactive sexual desire disorder. The results have been largely disappointing:
Physiological Response vs. Subjective Experience Studies consistently demonstrate that PDE5 inhibitors successfully increase genital blood flow in women. Using devices that measure vaginal pulse amplitude and lubrication, researchers have documented significant increases in these physiological markers of arousal when women take these medications.
However, when women are asked about their subjective experience—whether they feel more aroused, experience greater pleasure, or find sex more satisfying—the medications typically show no significant benefit compared to placebo.
The Disconnect: Why Blood Flow Isn’t Enough
This disconnect between physiological and psychological arousal reveals something important about female sexuality. Unlike the relatively linear relationship between genital blood flow and function in men (more blood flow = firmer erection = ability to have intercourse), female sexual response is considerably more complex.
Several factors contribute to this complexity:
1. The Role of Psychological Arousal Female sexual satisfaction appears to depend much more heavily on psychological factors including emotional connection, mental arousal, context, stress levels, relationship quality, and mood. Simply increasing blood flow to genital tissues does not address these psychological components.
2. Concordance Between Mind and Body Research on sexual concordance (the agreement between physical and mental arousal) shows that women typically have much lower concordance than men. A woman’s body may show physiological signs of arousal while her mind feels unaroused, or vice versa. Men generally show high concordance between genital response and subjective arousal.
3. Multiple Components of Sexual Response Female sexual dysfunction often involves multiple interrelated factors including desire, arousal, orgasm, pain, and satisfaction. Addressing blood flow alone targets only one small piece of this multifaceted puzzle.
Specific Conditions Where PDE5 Inhibitors Might Help Women
While general use in women has not proven beneficial, there are specific situations where these medications may offer some advantage:
1. Sexual Dysfunction Related to Antidepressants
Some studies suggest that PDE5 inhibitors may help counteract sexual side effects caused by selective serotonin reuptake inhibitors (SSRIs), though results are mixed. The medications may help improve physiological aspects of arousal that SSRIs impair.
2. Clitoral Blood Flow Issues
In cases where reduced clitoral sensation is specifically related to insufficient blood flow (rather than nerve damage or psychological factors), PDE5 inhibitors might theoretically provide benefit. However, this represents a small subset of female sexual dysfunction.
3. Postmenopausal Women
Some research has explored whether these medications might help address arousal difficulties in postmenopausal women experiencing changes in genital blood flow, though results remain inconclusive.
4. Women with Specific Medical Conditions
Conditions that affect blood flow systemically, such as diabetes or cardiovascular disease, might theoretically benefit from improved genital blood flow, though clinical evidence is limited.
Safety Considerations for Women
While Viagra and Cialis are generally well-tolerated, they are not without side effects:
Headaches
Flushing
Nasal congestion
Visual disturbances
Dizziness
Indigestion
More importantly, these medications are contraindicated in people taking nitrate medications (commonly prescribed for heart conditions) because the combination can cause dangerous drops in blood pressure.
Additionally, neither Viagra nor Cialis is FDA-approved for use in women. This means that any prescription would be off-label, and insurance typically would not cover the cost.
What Actually Helps Women with Sexual Dysfunction?
Given that PDE5 inhibitors generally don’t improve sexual satisfaction in women, what does work?
1. Addressing Psychological Factors
Sex therapy, cognitive behavioral therapy, and mindfulness-based approaches have shown significant benefit for many women with sexual difficulties. These therapies address the psychological components that play such a crucial role in female sexuality.
2. Hormone Therapy
For women experiencing sexual dysfunction related to hormonal changes (particularly during perimenopause and menopause), hormone replacement therapy or topical estrogen may help address vaginal dryness, pain, and atrophy.
3. FDA-Approved Medications for Women
Flibanserin (Addyi): Approved for premenopausal women with hypoactive sexual desire disorder, this medication works on neurotransmitter systems rather than blood flow
Bremelanotide (Vyleesi): An injectable medication also approved for low sexual desire in premenopausal women, working through melanocortin receptors
4. Treating Underlying Conditions
Addressing conditions that contribute to sexual dysfunction—such as depression, anxiety, relationship issues, chronic pain, or medication side effects—often proves more effective than attempting to treat the sexual symptoms directly.
5. Pelvic Floor Physical Therapy
For women experiencing pain during intercourse or difficulty with arousal related to pelvic floor dysfunction, specialized physical therapy can be remarkably helpful.
The Bottom Line
From a purely pharmacological perspective, PDE5 inhibitors like Viagra and Cialis do exactly what they’re designed to do in women: they inhibit the PDE5 enzyme, increase cGMP levels, promote smooth muscle relaxation, and enhance blood flow to genital tissues. The biochemical mechanism is sound, and the physiological effects are measurable.
However, improved blood flow does not translate to improved sexual sensitivity, pleasure, or satisfaction for most women. This reveals an important truth about human sexuality: the same biochemical pathway can have very different practical outcomes depending on the complex interplay of psychological, emotional, and social factors that influence sexual experience.
Female sexuality is not simply male sexuality in a different anatomical package. The relative importance of psychological versus physiological factors differs, and effective treatments must address this reality. For women experiencing sexual difficulties, a comprehensive approach that considers the full spectrum of physical, psychological, and relational factors is far more likely to help than a medication designed to address a primarily mechanical problem.
If you’re experiencing sexual difficulties, the most important first step is having an open conversation with a healthcare provider who can help identify the specific factors contributing to your concerns and develop a tailored treatment approach. While Viagra and Cialis probably won’t be part of that solution for most women, numerous other effective options exist.
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding medical questions, conditions, or treatment options.
Recent federal budget bills and policy decisions propose drastic cuts that would eliminate funding for critical scientific research at the National Institutes of Health (NIH) and various universities across the nation. While fiscal responsibility is important, these specific budgetary and policy decisions are not just penny-wise and pound-foolish; they are a direct threat to the health and well-being of every American.
The NIH is the largest biomedical research agency in the world, responsible for groundbreaking discoveries that have led to treatments for diseases ranging from cancer to Alzheimer’s, and the development of life-saving vaccines. Universities, often in partnership with NIH, are hotbeds of innovation, fostering the next generation of scientists and pushing the boundaries of medical knowledge. Gutting their funding is akin to dismantling our medical lifeline.
The Dire Consequences for Public Health:
Stifled Innovation and Delayed Cures: Imagine a future where the next breakthrough in cancer treatment, the vaccine for an emerging pandemic, or a more effective therapy for chronic diseases never sees the light of day. Without sustained funding, researchers cannot conduct the essential studies, trials, and investigations necessary to make these life-changing discoveries. We will simply stop making progress.
Brain Drain and Loss of Expertise: Our nation’s top scientists are drawn to environments where their work is supported and valued. If funding evaporates, we risk a significant “brain drain” as talented researchers seek opportunities in other countries that prioritize scientific advancement. This loss of expertise will have long-lasting, detrimental effects on our capacity to address future health challenges.
Increased Healthcare Costs: While it may seem counterintuitive, investing in preventative research and new treatments often reduces long-term healthcare costs. By understanding diseases better and developing more effective interventions, we can prevent serious illnesses, reduce hospital stays, and improve quality of life, ultimately saving billions in treatment expenses. Cutting research funding today will likely lead to far greater healthcare burdens tomorrow.
Weakened Pandemic Preparedness: The COVID-19 pandemic starkly illustrated the critical importance of robust scientific research for rapid response and vaccine development. Eliminating funding now would leave us dangerously vulnerable to future public health crises, effectively disarming us in the face of unknown pathogens.
Erosion of Public Trust and Global Leadership: America has long been a global leader in scientific discovery. Retreating from this commitment sends a troubling message to the world and undermines public trust in the ability of our institutions to protect citizens’ health.
Who Should Oppose These Moves?
The potential ramifications of these cuts are too significant to ignore. Everyone with an interest in a healthier future should actively oppose these budgetary decisions. This includes:
Patients and Patient Advocates: Those directly affected by diseases and their families, who rely on research for hope and new treatments.
Healthcare Professionals: Doctors, nurses, and other medical providers who understand the critical role research plays in advancing clinical care.
Scientists and Academics: The researchers themselves, who are on the front lines of discovery, and the institutions that house them.
Public Health Organizations: Groups dedicated to improving community health and preventing disease.
Concerned Citizens: Anyone who believes in the power of science to improve lives and secure a healthier future for all.
We cannot afford to mortgage our future health for short-sighted budget cuts. Contact your elected officials, support organizations advocating for scientific research, and make your voice heard. Our collective health depends on it.
If you’ve gone deep into the longevity and anti-aging rabbit hole, you’ve probably heard whispers about Epithalon (also spelled Epitalon)—a peptide that supposedly extends lifespan by acting on your cells’ internal aging clock. Unlike peptides that improve appearance or body composition, Epithalon claims to address aging at its most fundamental level: the shortening of your telomeres.
This sounds like science fiction, but Epithalon has over 30 years of Russian research behind it. So what is it really? How does it work? And can a simple four-amino-acid peptide actually slow down aging?
Let’s break down Epithalon—the peptide that targets the very mechanism of cellular aging.
The Discovery: Russian Longevity Research
The story of Epithalon begins in the Soviet Union during the Cold War era, when the USSR was heavily investing in gerontology (the study of aging) and life extension research.
Professor Vladimir Khavinson and the St. Petersburg Institute
In the 1970s-1980s, Professor Vladimir Khavinson at the St. Petersburg Institute of Bioregulation and Gerontology became obsessed with one question: What controls the aging process at the most fundamental level?
His hypothesis was controversial: he believed that the pineal gland—a small, pine-cone-shaped gland in your brain—was the master regulator of aging.
The Pineal Gland’s Role:
The pineal gland produces melatonin, which regulates your circadian rhythm (sleep-wake cycle). But Khavinson noticed something interesting: as people age, their pineal gland calcifies and produces less melatonin. This decline correlates strongly with other markers of aging.
He theorized that the pineal gland produces other regulatory peptides that control aging throughout the body, and that declining pineal function drives the aging process.
The Extraction and Synthesis
Khavinson’s team extracted peptides from the pineal glands of young calves. After years of fractionation and testing, they isolated a specific tetrapeptide (four amino acids) that had remarkable effects on lifespan in animal models.
They called it Epithalon (also known as Epithalamin when referring to the natural pineal extract).
The Results:
In animal studies spanning three decades, Epithalon demonstrated:
– 42% increase in lifespan in aged rats
– 27% increase in lifespan in fruit flies
– Extended lifespan in mice by normalizing age-related changes
– Restored reproductive function in old female rats
– Normalized circadian rhythms in aged animals
These weren’t subtle improvements—these were dramatic extensions of both lifespan and healthspan (years lived in good health).
The Mechanism: Telomeres and the Hayflick Limit
To understand how Epithalon works, you need to understand telomeres—the “aging clock” inside every cell.
What Are Telomeres?
Imagine your DNA as shoelaces. The plastic tips on the ends of shoelaces (aglets) prevent them from fraying. Telomeres are like those plastic tips—they’re protective caps on the ends of your chromosomes.
The structure:
Telomeres are repetitive DNA sequences (TTAGGG repeated thousands of times) that don’t code for any proteins. They’re essentially “junk” DNA whose only job is to protect the important genetic information on your chromosomes.
The Problem: Telomere Shortening
Every time a cell divides, the DNA replication machinery can’t quite copy all the way to the very end of the chromosome. A small piece of the telomere is lost with each division.
The Hayflick Limit:
In the 1960s, Dr. Leonard Hayflick discovered that normal human cells can only divide about 40-60 times before they stop. This is called the Hayflick Limit.
Why do they stop? Because their telomeres become critically short.
What happens when telomeres get too short:
1. Cellular senescence: The cell stops dividing and becomes a “zombie cell”—it’s alive but no longer functional. These senescent cells secrete inflammatory molecules that damage surrounding tissues.
2. Apoptosis: The cell dies (programmed cell death)
3. Genetic instability: If the cell tries to divide with critically short telomeres, chromosomes can fuse together or break, leading to cancer or cell death
This is why we age: Your cells can only divide a limited number of times. Eventually, you run out of functional cells, and tissues deteriorate.
The Solution: Telomerase
There’s an enzyme called telomerase that can add DNA sequences back onto telomeres, essentially “refilling” them.
Telomerase structure:
TERT (Telomerase Reverse Transcriptase): The protein enzyme component
TERC (Telomerase RNA Component): The RNA template that guides DNA synthesis
How it works:
Telomerase uses its RNA template to add TTAGGG repeats back onto chromosome ends, lengthening telomeres and allowing more cell divisions.
The catch: Most adult cells DON’T produce telomerase. It’s only active in:
Germ cells (sperm and eggs)
Stem cells
Some immune cells
Cancer cells (which is why they’re “immortal”)
This is your body’s anti-cancer defense mechanism. If all cells had active telomerase, they could divide forever—which is essentially what cancer is.
But it also means your normal cells have a built-in expiration date.
How Epithalon Works: Activating Telomerase
Here’s where Epithalon comes in. Research suggests it can activate telomerase in somatic cells (normal body cells) temporarily and safely.
The Molecular Mechanism
Step 1: Pineal Gland Stimulation
Epithalon appears to act directly on the pineal gland, stimulating it to produce more of its natural regulatory peptides and hormones, particularly melatonin.
The exact receptor mechanism isn’t fully characterized, but research suggests it binds to specific receptors on pinealocytes (pineal gland cells).
Step 2: Gene Expression Changes
Epithalon modulates the expression of genes involved in cellular aging and stress response. Specifically, it appears to:
Upregulate TERT gene expression (the telomerase enzyme)
Increase production of the telomerase enzyme
Enhance the enzyme’s activity
Step 3: Telomerase Activation
With more telomerase present and active, cells can add DNA sequences back onto their telomeres. This doesn’t make cells immortal—it just “resets” some of the telomere shortening that has occurred.
The evidence:
Studies on human cells in culture showed:
Telomere length increased by an average of ~10-15% after Epithalon treatment
Cells that had stopped dividing (senescent) could divide again
Lifespan of cells in culture extended by 20-40%
Step 4: Melatonin Normalization
Epithalon also normalizes melatonin production from the pineal gland. This has cascading effects:
Improved circadian rhythm
Better sleep quality
Enhanced antioxidant defenses (melatonin is a powerful antioxidant)
Improved neuroendocrine function
The Circadian Rhythm Connection
One of Epithalon’s most immediate effects is on circadian rhythm. The pineal gland releases melatonin in response to darkness, signaling your body that it’s time to sleep.
As you age:
Pineal gland calcifies
Melatonin production decreases
Circadian rhythm becomes less robust
Sleep quality deteriorates
Epithalon appears to “reset” the pineal gland, restoring more youthful melatonin patterns.
Why this matters for aging:
Your circadian rhythm controls hundreds of genes throughout your body. When it’s disrupted:
Immune function declines
Metabolic health worsens
Inflammation increases
Cognitive function deteriorates
By normalizing circadian rhythms, Epithalon may indirectly slow many aspects of aging.
The Antioxidant and Anti-Inflammatory Effects
Beyond telomeres and circadian rhythms, Epithalon has systemic effects on oxidative stress and inflammation.
Reducing Lipid Peroxidation
Lipid peroxidation is the “rusting” of fats in your body. Free radicals attack lipids in cell membranes, creating chain reactions that damage cells.
Oxidative damage accumulates with age and contributes to cardiovascular disease, neurodegeneration, and general tissue deterioration.
Normalizing Cortisol
Epithalon appears to normalize the hypothalamic-pituitary-adrenal (HPA) axis, which controls your stress response.
In aged animals, Epithalon:
Reduced elevated baseline cortisol
Improved cortisol response to stress (better stress adaptation)
Restored more youthful hormone patterns
Chronically elevated cortisol accelerates aging, so normalizing this is significant.
Practical Effects: What Users Report
Unlike peptides with immediate visible effects (like BPC-157 or GHK-Cu), Epithalon’s benefits are subtle and long-term. Here’s what users typically experience:
Effect 1: Improved Sleep Quality (Most Common, First to Notice)
Timeline: Within 3-7 days
Most users report:
Falling asleep more easily
Deeper, more restorative sleep
More regular sleep-wake cycle
Waking up more refreshed
Why: Melatonin normalization from pineal gland stimulation
This is often the only immediate, perceptible effect. Everything else is more subtle.
The Cancer Question: Is Telomerase Activation Safe?
This is the elephant in the room. If cancer cells use telomerase to become immortal, isn’t activating telomerase dangerous?
The Theoretical Concern
Cancer cells reactivate telomerase, allowing unlimited cell divisions. This is why they’re “immortal” and can form tumors.
If you artificially activate telomerase in normal cells, could you increase cancer risk?
Why Researchers Think Epithalon Is Safe
Reason 1: Temporary Activation
Epithalon activates telomerase briefly (10-20 days), not continuously. Cancer requires sustained telomerase activation.
Reason 2: Normal Cells Have Other Safeguards
Even with telomerase active, normal cells have multiple anti-cancer mechanisms:
p53 (tumor suppressor gene)
Cell cycle checkpoints
Immune surveillance
Cancer requires multiple mutations, not just telomerase.
Reason 3: 30+ Years of Animal Data
In animal studies, Epithalon didn’t increase cancer rates. In some studies, it actually reduced cancer incidence (possibly by improving immune function).
Reason 4: Clinical Use in Russia
Epithalon has been used in Russian clinics for decades without reported increases in cancer.
The Caveat
If you already have cancer (even undiagnosed), activating telomerase could theoretically accelerate tumor growth.
Recommendations:
Get appropriate cancer screenings before using Epithalon
Don’t use if you have active cancer
Monitor for any unusual symptoms
Consider it an “insurance policy” for healthy aging, not a treatment
Epithalon vs. TA-65: The Telomerase Wars
Epithalon isn’t the only telomerase activator on the market. TA-65 (a compound derived from astragalus root) is another option.
TA-65 (Astragalus Extract)
Mechanism: Activates telomerase through different pathway
Form: Oral capsules (no injections needed)
Dosing: Daily supplementation (250-1000 mg/day)
Evidence: Mixed results, some studies show telomere lengthening
Cost: $200-600/month (expensive)
Epithalon vs. TA-65 Comparison
Epithalon advantages:
More robust research (30+ years, multiple animal models)
More dramatic telomere lengthening in studies
Additional benefits (circadian rhythm, melatonin)
Cheaper ($50-150 per cycle, 2-4 cycles per year = $100-600/year)
TA-65 advantages:
Oral (no injections)
Commercially available and marketed legally
Some human clinical trial data
Continuous use (not cycles)
Verdict: Epithalon has more compelling research but requires injections. TA-65 is more convenient but weaker evidence and very expensive.
The Russian Connection: Pharmaceutical Availability
Epithalon is registered as a pharmaceutical drug in Russia under the brand name Endoluten.
In Russia:
Prescribed by doctors for age-related conditions
Used in longevity clinics
Covered by insurance in some cases
Extensive clinical use (thousands of patients)
In the US and Europe:
Not FDA-approved
Available as “research chemical”
Gray area legally
No pharmaceutical-grade version available
This creates quality control issues for Western users.
Side Effects and Safety Profile
Epithalon has an excellent safety profile in the research literature.
Reported Side Effects (Rare)
Injection-related:
Mild injection site discomfort
Rare: redness or itching
Systemic:
Temporary drowsiness (from melatonin increase)
Vivid dreams (melatonin effect)
Headache (rare, first few days)
No Significant Adverse Events:
No reported organ toxicity
No hormonal disruption
No significant drug interactions
No withdrawal or dependency
Contraindications
Avoid if you have:
Active cancer
History of retinoblastoma (rare eye cancer)
Autoimmune conditions (theoretical concern)
Pregnancy or breastfeeding (insufficient data)
Who Should Consider Epithalon?
Ideal Candidates
You might benefit if you:
Are 40+ years old (telomere shortening becomes significant)
Are focused on longevity and healthspan, not just appearance
Have family history of age-related diseases
Want to optimize cellular aging
Are willing to commit to long-term protocol (years)
Can afford periodic testing (telomere tests)
Especially valuable for:
Serious biohackers focused on lifespan extension
People with premature aging concerns
Those with poor sleep/circadian rhythm issues
Athletes interested in long-term health (not just performance)
Who Should Wait or Avoid
Don’t use if you:
Are under 30 (telomeres still long, pineal gland functional)
Have active cancer or history of cancer
Want immediate, visible results (wrong peptide for that)
Are unwilling to track biomarkers (how else will you know it’s working?)
Can’t commit to long-term approach
The Bottom Line: Is Epithalon the Real Deal?
Epithalon is one of the most scientifically intriguing anti-aging compounds available, but it’s also the hardest to evaluate subjectively.
What the science shows:
Activates telomerase and lengthens telomeres (in vitro and animal studies)
Extends lifespan in multiple animal models (20-40%)
Normalizes circadian rhythm and melatonin production
Reduces oxidative stress and inflammation
30+ years of Russian research and clinical use
What we don’t have:
Large-scale human randomized controlled trials
Long-term safety data in Western populations
FDA approval or pharmaceutical-grade sources
Direct evidence of human lifespan extension
The value proposition:
If you’re serious about longevity—actual extension of lifespan, not just looking good—Epithalon is one of the most compelling interventions available.
At $100-600 per year, it’s far cheaper than most longevity interventions. The risk appears low based on decades of use, and the potential upside (years added to your life) is enormous.
But this is a long game. You won’t see dramatic effects in weeks or months. This is about influencing the rate at which you age over years and decades.
For those playing the longevity game seriously, Epithalon deserves strong consideration. For those looking for quick results or cosmetic benefits, there are better options (like GHK-Cu or the Glow Stack).
Epithalon targets the aging clock itself. Whether it truly extends human lifespan remains to be proven definitively, but the evidence suggests it’s worth the bet.
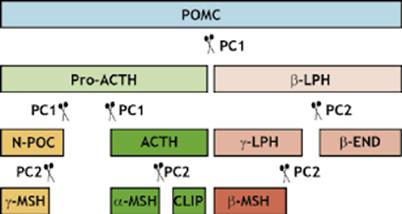
When most people hear “Melanotan 2,” they think of a tanning peptide. Some are aware it can enhance libido. But this understanding is like saying water is only for drinking—you’re missing everything else it does. Melanotan 2 (MT2) is actually a synthetic analog of alpha-melanocyte stimulating hormone (α-MSH), a regulatory neuropeptide signaling molecule that interfaces with one of the body’s most fundamental biological control systems: the melanocortin system.
What makes MT2 fascinating isn’t what it does to your skin. It’s what it does to the underlying biological architecture that separates health from disease. For biohackers and those interested in longevity and wellness, understanding MT2 requires understanding how the melanocortin system functions as a master regulatory network controlling inflammation, metabolism, and energy production throughout your entire body.
Understanding Alpha-MSH and the Melanocortin System
The Genesis of Alpha-MSH
Cleavage of POMC by PCs (Prohormone Convertases)
Alpha-MSH originates from pro-opiomelanocortin (POMC) neurons, primarily located in the arcuate nucleus of the hypothalamus. POMC is cleaved by prohormone convertases to produce several bioactive peptides, including:
Alpha-MSH (α-MSH)
Beta-MSH (β-MSH)
Adrenocorticotropic hormone (ACTH)
Beta-endorphin
Alpha-MSH itself is a tridecapeptide (13 amino acids) derived from ACTH. The native pathway begins when POMC neurons detect signals related to energy balance, immune activation, or inflammatory status. Upon activation, these neurons release α-MSH into various brain regions and the bloodstream, where it acts as a signaling molecule across multiple organ systems.
The Melanocortin Receptors: A Distributed Network
Here’s where the biology becomes profound. Alpha-MSH and its analogs like MT2 don’t just bind to melanocytes in your skin. They bind to melanocortin receptors (MC1R through MC5R) distributed throughout your entire body:
MC1R – Found on melanocytes (skin pigmentation), also expressed on immune cells MC3R – Primarily in adipose tissue and hypothalamus (energy homeostasis, inflammation) MC4R – Hypothalamus, brainstem, throughout CNS (appetite regulation, energy expenditure, sexual function) MC5R – Widely distributed in peripheral tissues including sebaceous glands and immune cells
The critical insight from research at institutions like the University of Arizona (2011) was discovering that these receptors are located precisely where human biology encounters inflammatory problems or metabolic dysfunction. They’re in endothelial cells, kidneys, immune cells, myocardium, the brain’s reward centers, digestive system, and metabolic tissues.
This isn’t coincidental; it’s architectural. The melanocortin system evolved as a master regulatory system for coordinating responses across multiple physiological domains simultaneously.
The Three Biological Failures: A Framework for Understanding Disease
Modern chronic diseases—type 2 diabetes, cardiovascular disease, neurodegeneration, autoimmune conditions—all converge through three fundamental biological failure points:
Systemic Inflammation – Chronic inappropriate activation of inflammatory cascades
Metabolic Dysfunction – Insulin resistance and impaired cellular energy metabolism
Energy Failure – Mitochondrial dysfunction and insufficient ATP production
What makes MT2 scientifically compelling is that through melanocortin receptor optimization, it addresses all three simultaneously. Your body isn’t compartmentalized; it’s a unified electromagnetic biochemical information system. When you understand that MT2 activates melanocortin receptors across multiple organ systems at once, you realize it’s not about treating isolated symptoms but optimizing fundamental biological systems.
Systemic Inflammation: The Master Switch
The Inflammatory Cascade
In the modern environment, processed foods, endotoxin exposure, hyperglycemia, oxidative stress, circadian disruption, our immune systems exist in a state of chronic, inappropriately high activation. Macrophages are hypervigilant, dendritic cells are overstimulated, and the T-helper cell TH1/TH17 populations are expanded. This creates a state of smoldering inflammation that slowly damages tissue integrity across all organ systems.
IL-17 – TH17-secreted cytokine linked to autoimmune conditions
NFκB (Nuclear Factor kappa B) is the master transcription factor that amplifies this inflammatory cascade. When activated, it triggers production of more inflammatory cytokines, creating a self-perpetuating cycle.
How MT2 Suppresses Inflammation
MT2’s anti-inflammatory mechanism operates through several pathways:
POMC Neuron Activation: Research from Stanford University (2015) demonstrated that POMC neuron activation specifically suppresses NFκB in peripheral tissues. By releasing α-MSH directly into the hypothalamic-pituitary-adrenal (HPA) axis, MT2 essentially turns off the biological switch that drives 95% of chronic disease processes.
Immune Cell Modulation: MT2 stimulates MC3R and MC4R on macrophages and dendritic cells, shifting the immune response from a pro-inflammatory (TH1/TH17-dominant) state to an anti-inflammatory, regulatory (TH2/T-reg-dominant) state.
Direct Cytokine Suppression: A study in the 2012 Journal of Immunology study showed that melanocortin stimulation directly inhibits TNF-α, IL-6, and IL-1β production in activated macrophages. A 2014 University of Washington study demonstrated that α-MSH-mediated MC4R signaling decreased IL-6, TNF-α, and IL-17 production by approximately 70% in human blood mononuclear cells; not rat studies, but human data.
This isn’t symptomatic suppression. You’re biochemically rebalancing the immune system toward tolerance and away from chronic violent activation.
Insulin resistance isn’t about insufficient insulin production; Rather, it’s about cells becoming deaf to insulin signaling. This happens through multiple mechanisms:
Inflammatory Damage to IRS-1: Chronic inflammation damages insulin receptor substrate-1 (IRS-1) signaling in muscle cells, preventing insulin from activating glucose uptake pathways
Lipid Accumulation: Excess fatty acid accumulation in mitochondria impairs glucose oxidation, creating a metabolic traffic jam
AGE Formation: Chronic hyperglycemia drives formation of advanced glycation end products (AGEs), which activate RAGE receptors and trigger NFκB, perpetuating inflammation
Mitochondrial Dysfunction: Reduced ATP production prevents the energy-dependent steps of glucose metabolism from functioning properly
MT2’s Multi-Mechanism Metabolic Restoration
Mechanism 1 – Inflammatory Resolution: By suppressing systemic inflammation, MT2 reduces SOCS (suppressor of cytokine signaling) proteins that phosphorylate and inactivate IRS-1. Your insulin signal becomes cleaner and more effective at the receptor level.
Mechanism 2 – Enhanced Fat Oxidation: MT2 stimulates MC4R in the sympathetic nervous system, increasing metabolic rate and fatty acid oxidation. This reduces intramuscular lipid accumulation, allowing mitochondria to process glucose more efficiently.
Mechanism 3 – Reduced AGE Formation: By reducing NFκB activation, MT2 decreases AGE formation and RAGE signaling, improving glucose metabolism directly.
Mechanism 4 – AMPK Activation: Research from the Journal of Molecular Endocrinology (2013) demonstrated that melanocortin pathway activation increases AMPK (AMP-activated protein kinase) phosphorylation in skeletal muscle. AMPK is the cellular energy sensor that tells mitochondria to produce more ATP and metabolize glucose more efficiently.
The result isn’t just lower blood sugar—it’s fundamentally improved cellular responsiveness to insulin at the molecular level. Duke University (2015) showed that POMC neuron activation increases metabolic rate by 22% through sympathetic-mediated increases in brown adipose tissue activity and mitochondrial uncoupling protein expression.
Energy Production: The Mitochondrial Foundation
The Invisible Pandemic
Mitochondrial dysfunction is the invisible pandemic underlying most chronic disease. Modern life—high-carbohydrate processed foods, circadian disruption, chronic stress, toxin exposure—systematically damages mitochondrial function. When mitochondria are impaired, everything breaks:
Insufficient ATP for synaptic transmission and memory consolidation
Impaired myelin maintenance in neurons
Reduced protein synthesis capacity
Inability to maintain cellular ion gradients
Compromised detoxification pathways
The symptoms manifest differently depending on which tissues are most affected, but the root cause is the same: energy failure.
MT2’s Mitochondrial Optimization
Sympathetic Activation: MT2 increases metabolic rate and upregulates mitochondrial biogenesis through PGC-1α (peroxisome proliferator-activated receptor gamma coactivator 1-alpha) activation. You’re literally creating more and healthier mitochondrial power plants.
Reduced Oxidative Stress: By decreasing inflammation, MT2 reduces production of mitochondrial-damaging reactive oxygen species (ROS) and pro-inflammatory cytokines that downregulate mitochondrial proteins. Research suggests this can reduce the normal ~60% ATP deficit seen in inflammatory states.
Improved Substrate Utilization: MT2’s enhancement of insulin signaling allows for better glucose oxidation within mitochondria, providing optimal fuel for the electron transport chain and ATP synthesis.
System-by-System Analysis
Cardiovascular System: Endothelial Regeneration
Your endothelium, the single-cell layer lining your arteries,is responsible for:
Nitric oxide (NO) production and vasodilation
Anti-coagulation and anti-inflammation
Vascular tone regulation
Filtering inflammatory molecules
Endothelial dysfunction occurs through chronic inflammation (inflammatory molecule penetration), oxidative stress (reduced NO bioavailability), and insulin resistance (impaired endothelial mitochondrial function). This leads to oxidized LDL particles activating scavenger receptors on macrophages, foam cell formation, and atherosclerosis.
Reduces baseline sympathetic tone through cortisol and norepinephrine normalization
A study in Circulation Research (2011) showed that melanocortin agonism improved endothelial function and reduced atherosclerotic plaque formation. Your cardiovascular system regenerates when inflammation decreases and mitochondrial function improves.
Renal System: Protecting Filtration
Kidneys are highly metabolically active organs with massive energy requirements. Kidney disease progresses through:
Improved reabsorption of filtered glucose and amino acids
A study in the American Journal of Nephrology (2014) demonstrated that melanocortin pathway activation reduced proteinuria and improved glomerular filtration rate by 57% in diabetic nephropathy models.
Nervous System: Neuroprotection and Neuroregeneration
The brain is approximately 60% lipids, requires constant ATP, has limited blood supply, and is exquisitely sensitive to inflammation. When systemic inflammation is present, microglial cells (the brain’s immune cells) enter a state of chronic hyperactivation.
These cytokines damage synaptic connections, impairing long-term potentiation
Promotion of amyloid-beta aggregation (foundational to Alzheimer’s)
Reduced brain-derived neurotrophic factor (BDNF)
Increased oxidative stress
MT2’s Neuroprotective Mechanisms:
Anti-inflammatory Effects: MT2 crosses the blood-brain barrier and suppresses microglial activation through melanocortin receptor signaling. The Journal of Neuroinflammation (2012) showed that α-MSH decreased microglial TNF-α and IL-6 production by approximately 70%.
Enhanced ATP Production: By improving mitochondrial function systemwide, MT2 ensures the brain has sufficient energy for optimal neurotransmission and synaptic plasticity.
Insulin Sensitivity: By improving systemic insulin sensitivity, MT2 enhances neuronal glucose uptake and metabolism, critical for cognitive function.
Applications to Neurodegenerative Disease
Alzheimer’s Disease: Begins with neuroinflammation and amyloid-beta accumulation creating a vicious cycle. MT2 suppresses microglial activation, reduces neuroinflammation, and reduces amyloid-beta-induced inflammatory amplification. Neurobiology of Aging (2013) showed MT2 reduced amyloid-beta-induced microglial TNF-α production.
Parkinson’s Disease: Characterized by selective dopaminergic neuron loss in the substantia nigra, driven by neuroinflammation and mitochondrial dysfunction. MT2 suppresses the neuroinflammation damaging dopaminergic neurons, improves mitochondrial function in remaining neurons, and reduces alpha-synuclein aggregation downstream.
Multiple Sclerosis: An autoimmune condition where the immune system attacks myelin, driven by TH17 overactivity and insufficient T-regulatory cell activity. MT2 shifts the immune response from TH1/TH17 toward TH2/T-reg, reducing the myelin-directed attack and promoting remyelination by oligodendrocytes. The Journal of Neuroinflammation (2014) showed melanocortin agonism increased regulatory T cells and decreased TH17 activity in MS.
Sexual Function: The Complete Biological Picture
Erectile dysfunction and low libido are fundamentally about impaired biological systems, not pharmaceutical deficiencies.
The Requirements for Proper Sexual Function:
Cavernosal smooth muscle relaxation (blood fills corpus cavernosum)
Penile arterial vasodilation (blood flows in)
Central arousal signals from the brain (system activation)
Where Modern Men Break Down:
Chronic stress: Elevated cortisol and norepinephrine create sympathetic dominance—the penis is stuck in fight-or-flight mode, unable to relax smooth muscle
Chronic inflammation: Elevated TNF-α, IL-6, IL-17 cause endothelial dysfunction, reduced nitric oxide production, and impaired vasodilation
Metabolic dysfunction: Reduced ATP in smooth muscle cells means insufficient energy to maintain the relaxation required for erection
MT2’s Multi-Level Sexual Enhancement:
Brain Level: MT2 stimulates melanocortin receptors in the medial preoptic area (MPOA) and paraventricular nucleus (PVN)—the brain’s sexual arousal centers. University of Amsterdam research (2007) showed direct melanocortin agonism in the PVN increases penile erection frequency and intensity by 47%. MT2 also increases dopamine and oxytocin in these regions, fundamental to sexual motivation and desire.
Endothelial Level: MT2 suppresses systemic inflammation, improves NO production in endothelial cells, and increases cyclic GMP in cavernosal smooth muscle cells, the biological cascade for vasodilation and blood flow.
Sympathetic Level: By suppressing systemic inflammation (the chronic stressor), MT2 reduces baseline norepinephrine and cortisol, normalizing sympathetic nervous system tone and releasing the fight-or-flight grip on genital tissue.
Mitochondrial Level: By improving ATP production in smooth muscle cells, MT2 ensures sufficient energy to maintain the metabolic state that smooth muscle relaxation requires.
The critical distinction: The International Journal of Impotence Research (2009) showed melanocortin agonism produces durable improvements in erectile function long after discontinuation. You’re not masking symptoms, you’re fixing the underlying biology.
Clinical Considerations and Dosing Principles
Understanding the Holistic Effect
A crucial principle: When you take MT2, you don’t get to choose which melanocortin receptors it activates. Unlike targeted drugs that force specific responses, peptides work through your body’s existing regulatory pathways. MT2 activates the entire melanocortin system, you receive all the effects simultaneously.
This is fundamentally different from pharmaceutical drugs. Drugs act like wrecking balls, forcing your body to respond even against its natural regulatory mechanisms. Peptides can only tell your body to do what it’s already designed to do—they make these natural processes work orders of magnitude better but cannot force unnatural responses.
The Integration Approach
MT2 is not a magic bullet or a supplement to add to an existing stack without consideration. The most effective approach:
Address Foundation First: Optimize diet, sleep, circadian rhythm, and movement patterns
Strategic Peptide Integration: Introduce MT2 as part of a comprehensive approach to biological optimization
Monitor and Adjust: Track inflammatory markers (hsCRP), metabolic markers (fasting insulin, HbA1c), and functional outcomes
Dosing Framework
Typical research dosing ranges from 0.25mg to 1mg, but individual response varies significantly based on:
Baseline melanocortin receptor sensitivity
Current inflammatory status
Metabolic health status
Body composition
Start low (0.25mg) and assess response over 2-3 weeks before adjusting. The goal isn’t to maximize tanning or achieve a specific aesthetic outcome—it’s to optimize the melanocortin system for comprehensive health benefits.
Broader Implications: A Systems Biology Perspective
Why This Matters for Longevity
The aging process is fundamentally characterized by:
Progressive accumulation of inflammatory damage
Declining mitochondrial function and biogenesis
Increasing insulin resistance and metabolic inflexibility
Loss of regenerative capacity
MT2 addresses each of these aging hallmarks through melanocortin system optimization. By maintaining proper inflammatory regulation, metabolic function, and energy production, you’re not just treating age-related diseases, you’re intervening in the aging process itself.
The Paradigm Shift
Modern medicine compartmentalizes: dermatologists for skin, cardiologists for heart, neurologists for brain. But your body doesn’t recognize these arbitrary divisions. It’s a unified system where dysfunction in one area cascades to affect all others.
The melanocortin system represents a biological master controller coordinating responses across these arbitrary medical specialties. Understanding and optimizing this system requires thinking in terms of:
Systems biology rather than reductionist medicine
Root cause resolution rather than symptom management
Biological optimization rather than pharmaceutical intervention
Research Directions
Current research is exploring melanocortin receptor targeting for:
Type 2 diabetes and metabolic syndrome
Cardiovascular disease and atherosclerosis
Neurodegenerative diseases
Autoimmune conditions
Chronic kidney disease
Cancer-related cachexia
The National Institutes of Health (2013) confirmed that the melanocortin pathway is fundamentally involved in regulating systemic inflammation through POMC neurons, metabolic homeostasis through HPA axis regulation, immune function through cytokine modulation, sexual function through brain receptor activation, cardiovascular tone through endothelial signaling, and cognitive function through hippocampal and prefrontal cortex expression.
Conclusion: Beyond the Surface
Melanotan 2 is not a tanning peptide with some side benefits. It’s not primarily a libido enhancer. It’s an intervention into one of the body’s fundamental regulatory systems, the melanocortin system that controls the three biological levers separating health from disease.
Every chronic disease—cardiovascular disease, type 2 diabetes, Alzheimer’s, Parkinson’s, multiple sclerosis, kidney disease, erectile dysfunction, cognitive decline—bottlenecks through the same three mechanisms: systemic inflammation, metabolic dysfunction, and energy failure. MT2, through its activation of melanocortin receptors across multiple organ systems, addresses all three simultaneously.
This is what happens when you stop treating symptoms and start optimizing fundamental biological systems. When MC4 receptors optimize sympathetic tone and metabolic rate, when AMPK activates in muscle tissue restoring insulin sensitivity, when POMC neurons suppress NFκB and TNF-α throughout the body, when macrophages shift from pro-inflammatory to anti-inflammatory phenotypes, when mitochondria regenerate and produce more ATP with less oxidative stress—you’re not treating a disease. You’re fixing the biological architecture that allows disease to exist.
For biohackers and those serious about longevity, understanding MT2 means understanding that health is not the absence of disease but the presence of optimized biological function. The melanocortin system is the master lever. MT2 is the tool to optimize it.
The question isn’t whether MT2 can tan your skin or enhance libido. The question is: what happens when you solve the system that regulates inflammation, metabolism, and energy production across your entire body? The answer is written in the research, confirmed by the biochemistry, and increasingly validated by clinical outcomes.
This is the future of medicine—not managing symptoms with pharmaceuticals, but optimizing biological systems with our own regulatory molecules. For those willing to understand the science, MT2 represents a glimpse into what’s possible when we work with biology rather than against it.
Note: This article presents scientific research and biological mechanisms for educational purposes. MT2 is a research peptide, and any therapeutic use should be undertaken with qualified medical supervision. Individual responses vary based on health status, genetics, and other factors. The information presented is for educational purposes and should not be construed as medical advice.
For decades, thousands of LGBTQ individuals were subjected to treatments designed to change their sexual orientation or gender identity. Known as conversion therapy, reparative therapy, or ex-gay therapy, these practices represent one of the darker chapters in modern mental health care. Understanding this history is crucial to preventing its continuation and protecting vulnerable LGBTQ youth today.
What Is Conversion Therapy?
Conversion therapy encompasses a range of practices aimed at changing, suppressing, or “curing” a person’s sexual orientation or gender identity. These interventions have taken many forms over the years—from psychoanalysis and behavioral conditioning to religious counseling and, in extreme historical cases, aversive techniques including electroshock therapy and nausea-inducing drugs. The underlying premise has always been the same: that being gay, lesbian, bisexual, or transgender is a disorder that can and should be treated.
Practitioners have employed various methods, including talk therapy sessions focused on identifying supposed childhood trauma or family dysfunction that “caused” homosexuality, behavioral modification techniques, prayer and religious intervention, and group therapy designed to reinforce heterosexual identity. Some approaches were clinical, conducted by licensed therapists, while others operated within religious organizations with little to no mental health training.
The Origins and Rise of Conversion Therapy
The concept of homosexuality as a treatable condition emerged from early 20th-century psychiatry, when same-sex attraction was classified as a mental illness. Sigmund Freud himself had a complex view on the matter, while he considered homosexuality a developmental arrest, he famously wrote to a mother in 1935 that it “is nothing to be ashamed of, no vice, no degradation” and expressed skepticism about conversion efforts.
Nevertheless, his followers were less cautious. Post-World War II America saw an intensification of efforts to “cure” homosexuality. Psychoanalysts claimed they could redirect sexual orientation through long-term therapy exploring family relationships and childhood experiences. The 1950s and 1960s brought increasingly aggressive approaches, including aversion therapy—shocking patients or inducing vomiting while showing them same-sex imagery.
Conversion therapy reached its mainstream peak in the 1970s and early 1980s, paradoxically just as the gay rights movement was gaining momentum. Even after the American Psychiatric Association removed homosexuality from its Diagnostic and Statistical Manual of Mental Disorders in 1973, many practitioners continued offering these treatments, now framing them as helping people whose sexuality conflicted with their religious values or personal desires.
Promised Results Versus Reality
Proponents of conversion therapy made bold claims. They reported success rates ranging from 30% to 70%, asserting that motivated individuals could achieve heterosexuality through dedicated treatment. Organizations published testimonials from supposedly “ex-gay” individuals who claimed to have successfully changed their orientation and found happiness in heterosexual marriages.
The reality told a starkly different story. Rigorous scientific examination revealed that these claimed successes were largely illusory. Most studies supporting conversion therapy suffered from severe methodological flaws: they lacked control groups, relied on self-reporting without objective measures, defined “success” vaguely (often meaning merely behavioral change or suppression rather than orientation change), and failed to conduct long-term follow-up.
When researchers looked more closely, they found that many “success” stories involved people who had simply learned to suppress their attractions or who were bisexual to begin with. The claimed changes typically proved temporary. Numerous individuals who had been touted as conversion therapy success stories later came forward to acknowledge they remained gay and had only learned to hide or deny their true selves.
The recidivism rate was devastating. Studies that did conduct follow-ups found that the vast majority of people who underwent conversion therapy eventually acknowledged that their sexual orientation had not changed. Many who initially claimed success later returned to living openly as LGBTQ individuals, often after years of internal struggle and failed attempts to maintain a heterosexual identity.
The Harm Caused
Far from being merely ineffective, conversion therapy proved actively harmful. Research documented serious negative outcomes including depression, anxiety, decreased self-esteem, substance abuse, homelessness (particularly among youth rejected by families), social isolation, difficulty with intimacy and relationships, post-traumatic stress disorder, and suicidal ideation and attempts.
The psychological damage stemmed from the therapy’s fundamental premise: that something core to a person’s identity is broken and shameful. Participants internalized the message that they were defective, leading to profound shame and self-hatred. Many described feeling they had failed when the therapy didn’t “work,” adding guilt to their existing distress. The process of trying to suppress or deny one’s authentic self created lasting psychological wounds.
For minors subjected to conversion therapy—often at their parents’ insistence—the harm was particularly acute. Young people reported feeling betrayed by caregivers, isolated from peers, and fundamentally broken. Some were sent to residential programs that combined conversion therapy with other abusive practices. The suicide rate among LGBTQ youth who underwent conversion therapy was found to be significantly elevated compared to those who did not.
Exodus International and the Ex-Gay Movement
No organization embodied the conversion therapy movement more than Exodus International. Founded in 1976, Exodus became the largest ex-gay ministry in the world, with affiliated churches and counseling centers across North America and beyond. The organization promoted the message that through Christian faith and therapy, people could leave homosexuality behind.
Exodus leaders appeared on television, published books, and lobbied against LGBTQ rights legislation, citing their existence as proof that being gay was a choice. They offered hope to religious families struggling to reconcile their faith with their children’s sexual orientation, and to LGBTQ individuals tormented by religious teachings that condemned them.
The scandals that eventually surrounded Exodus were numerous and devastating. Multiple Exodus leaders and spokespeople who had claimed to be “ex-gay” were later discovered in same-sex relationships. John Paulk, once the poster child for the ex-gay movement whose story was featured in national advertising campaigns, eventually acknowledged he was still gay and renounced conversion therapy. Michael Bussee, a co-founder of Exodus, left the organization in 1979, came out as gay, and became a vocal critic of the movement.
In 2012, Alan Chambers, then president of Exodus International, made a stunning admission: the majority of people who went through Exodus programs had not experienced a change in their sexual orientation. He acknowledged the harm the organization had caused. In June 2013, Chambers issued a formal apology to the LGBTQ community and announced that Exodus International would shut down. “I am sorry for the pain and hurt many of you have experienced,” he wrote. “I am sorry that some of you spent years working through the shame and guilt you felt when your attractions didn’t change.”
The closure of Exodus represented a watershed moment, but it did not end conversion therapy. Many former Exodus affiliates continued operating independently, and new organizations emerged to fill the void.
Professional Opposition and Scientific Consensus
As evidence of harm mounted, professional mental health organizations took increasingly firm stands against conversion therapy. The American Psychiatric Association led the way, stating in 2000 that conversion therapy can cause depression, anxiety, and self-destructive behavior. Their position paper emphasized that homosexuality is not a mental disorder and does not require treatment.
The American Psychological Association conducted a comprehensive review of research in 2009, concluding that conversion therapy was unlikely to be successful and carried significant risk of harm. They advised mental health professionals to avoid telling clients they could change their sexual orientation through therapy. The American Medical Association, American Academy of Pediatrics, American Counseling Association, National Association of Social Workers, and numerous other professional organizations issued similar statements.
These organizations affirmed that sexual orientation is not a choice and is not changeable through therapeutic intervention. They emphasized that the appropriate therapeutic response to a client struggling with their sexual orientation is to help them accept themselves, not to attempt to change them. The scientific consensus became clear and overwhelming: conversion therapy is neither ethical nor effective.
Legislative Battles
The fight over conversion therapy moved into legislative arenas as LGBTQ advocates sought legal protections, particularly for minors. California became the first state to ban conversion therapy for minors in 2012, followed quickly by New Jersey in 2013. These laws prohibited licensed mental health professionals from practicing conversion therapy on patients under 18.
The legislative efforts sparked fierce opposition. Religious organizations and conservative groups argued that such bans violated parental rights, religious freedom, and free speech. Legal challenges were mounted in multiple states, with opponents claiming that conversion therapy bans prevented therapists from helping clients who voluntarily sought to change their orientation.
Courts generally upheld the bans. In 2014, the Ninth Circuit Court of Appeals ruled that California’s law was constitutional, finding that the state had a legitimate interest in protecting minors from harmful practices. The Supreme Court declined to hear appeals, letting the ruling stand.
The momentum built gradually but persistently. By 2025, numerous states, the District of Columbia, and Puerto Rico had enacted similar protections. Many municipalities in states without statewide bans passed local ordinances. The bans typically applied only to licensed professionals working with minors, leaving religious counseling and services for adults largely unregulated, a compromise that allowed passage while leaving some activists unsatisfied.
However, the battle was far from one-sided. Some states introduced “anti-ban” legislation seeking to protect the practice of conversion therapy as a form of religious or therapeutic freedom. These efforts reflected ongoing cultural divisions over LGBTQ rights and the role of government in regulating healthcare and religious practices.
Where Things Stand Today
Conversion therapy exists in a state of contested territory. While banned for minors by licensed professionals in many jurisdictions, it continues in various forms: unlicensed religious counseling, life coaching that falls outside professional regulation, practices in states without protective legislation, and services for adults who voluntarily seek them.
The professional mental health community remains united in opposition. Major therapeutic organizations continue to condemn the practice and call for comprehensive bans. Research continues to document harm, with particular concern for vulnerable populations including LGBTQ youth, people in religious communities that condemn homosexuality, and individuals in countries where being LGBTQ is criminalized.
Internationally, the picture is mixed. Some countries, including Brazil, Ecuador, and Malta, have banned conversion therapy. The United Nations and World Health Organization have called for global bans. However, in many parts of the world, conversion therapy not only continues but thrives, often with government support or in societies where LGBTQ identities remain deeply stigmatized.
The legacy of conversion therapy serves as a sobering reminder of how prejudice can masquerade as treatment and how good intentions—whether from families or even some practitioners—can enable profound harm when built on flawed premises. For LGBTQ individuals, particularly those who survived these interventions, the scars often remain.
Moving forward, the focus has shifted toward affirmative therapy—approaches that help LGBTQ individuals accept themselves, cope with minority stress and discrimination, and build authentic lives. The question is no longer whether sexual orientation can be changed, but how to support people in thriving as their authentic selves.
The story of conversion therapy is ultimately about the human cost of treating identity as pathology. It stands as a cautionary tale for mental health care and a reminder that scientific evidence and human dignity must guide therapeutic practice, not cultural prejudice or wishful thinking.