By the time principal dancer Misty Copeland announced her retirement and shared a candid video of her post-surgical recovery — appearing to show rehabilitation following hip surgery — the ballet world had witnessed what many already understood: that a career at the pinnacle of classical dance exacts a profound physical cost. Copeland, who made history as the first African American female principal dancer at American Ballet Theatre, danced through injuries that would have ended most careers. Her public recovery pulled back the curtain on a reality that elite ballerinas know intimately but rarely discuss: the human body was not designed for the demands of professional ballet, and it pays dearly for decades of attempting the impossible.

While audiences marvel at the effortless grace of a ballerina suspended en pointe, orthopedic surgeons see something else: a skeleton stressed beyond its anatomical limits, joints compressed at angles evolution never intended, and connective tissue in a perpetual state of micro-trauma. The foot and ankle injuries associated with pointe work are well known, but they represent only part of the story. From the lumbar spine to the hip socket, from the knee to the sacroiliac joint, ballet extracts damage at every level of the musculoskeletal system.
The Hip: Ballet’s Most Demanding Joint
The hip is ground zero for the kind of catastrophic wear that Copeland’s recovery video seemingly illustrates. Ballet’s foundational aesthetic principle — turnout, the external rotation of both legs from the hip socket — places extraordinary demands on the acetabular labrum, the ring of cartilage that deepens the hip socket and stabilizes the femoral head. Elite dancers spend years forcing their hips into ranges of rotation that exceed what the joint anatomy typically allows, and the labrum bears the brunt of this.
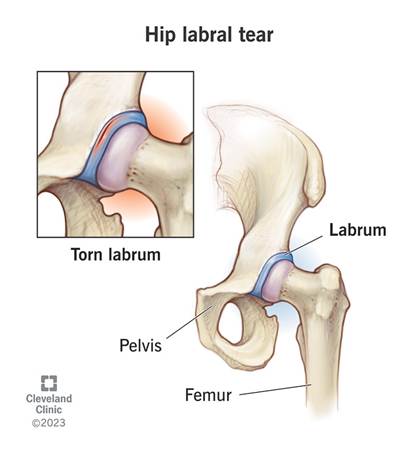
Labral tears are endemic among professional ballet dancers. Studies suggest rates as high as 80 to 90 percent among elite dancers who undergo hip imaging, though many tears remain asymptomatic until the cumulative damage reaches a tipping point. When symptoms emerge — deep groin pain, a clicking or catching sensation, pain with hip flexion or external rotation — they signal structural compromise that often requires surgical intervention, typically arthroscopic labral repair or reconstruction.

Beyond labral pathology, elite dancers are susceptible to femoroacetabular impingement (FAI), a condition in which bony prominences on the femoral head or acetabular rim create abnormal contact during movement. The forced extremes of ballet — deep plié, grand battement, arabesque — grind these surfaces together repeatedly, producing progressive cartilage erosion that can lead to early-onset osteoarthritis of the hip. Some former dancers undergo total hip replacement in their forties, decades earlier The Knee: Bearing the Load of Every Landing
Every jump in ballet ends with a landing and the knee absorbs the shock. In professional ballet, a dancer may execute hundreds of jumps per rehearsal day, each one concentrating forces of three to five times body weight through the knee joint. Over a career spanning fifteen to twenty years at the professional level, this cumulative loading creates predictable patterns of injury and degeneration.
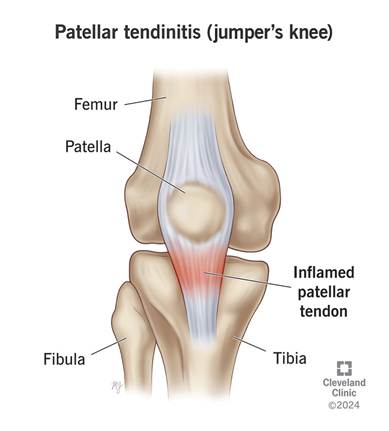
Patellar tendinopathy, colloquially known as jumper’s knee, is one of the most common overuse injuries in ballet. The repeated eccentric loading of the quadriceps during landing produces microtrauma within the patellar tendon that, if insufficiently recovered, progresses to chronic tendon degeneration. Anterior knee pain from patellofemoral syndrome is equally prevalent, arising partly from the external rotation demands of turnout, which alter the tracking mechanics of the patella and increase lateral compartment pressure.
Meniscal damage follows a similar pattern to hip labral tears: gradual wear that accumulates invisibly until a threshold is crossed. The medial and lateral menisci, which act as shock absorbers and stabilizers within the knee, are subject to compressive and shear forces during the deep plié positions ballet demands. Partial meniscal tears, once managed conservatively, may ultimately require surgical intervention and frequently herald early-onset knee osteoarthritis.
The Spine: Dancing Through Compression and Instability
The demands placed on a ballerina’s spine are contradictory and unforgiving. Ballet simultaneously requires extreme lumbar extension, the arched back of an arabesque and the postural discipline of a perfectly vertical torso in fifth position. This oscillation between hyperlordosis and strict alignment, repeated across thousands of hours of training, creates a unique spinal stress profile.
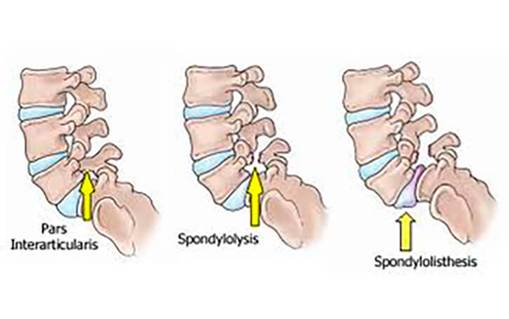
Spondylolysis, a stress fracture of the pars interarticularis, a small bridge of bone between vertebral facet joints, occurs at significantly elevated rates among ballet dancers compared to the general population. The repetitive hyperextension of arabesque and attitude positions creates cyclical stress at the posterior elements of the lumbar spine, particularly at L4 and L5. Bilateral spondylolysis can progress to spondylolisthesis, in which a vertebra slips forward relative to the one below it, causing chronic back pain and nerve root compromise.

Intervertebral disc pathology is also common, driven both by the compressive loads of partnering, where male dancers lift ballerinas repeatedly overhead, and by the chronic postural demands of training. Herniated discs, most frequently at L4-L5 and L5-S1, can produce radiculopathy that radiates down the leg, threatening not just a dancer’s comfort but her technical capability and career longevity.
The Foot and Ankle: Where Dance Meets Damage
No discussion of ballet injuries is complete without the foot, and though this territory is well mapped, its severity bears emphasis. Dancing en pointe, the practice of supporting the full body weight on the tips of the toes, is perhaps the most anatomically radical thing a human being can routinely do. The metatarsophalangeal joints, the sesamoid bones beneath the first metatarsal, and the entire bony architecture of the forefoot are subjected to loading conditions that have no parallel in normal human movement.

Hallux valgus — the lateral deviation of the great toe, is nearly universal among female ballet dancers who have danced on pointe for many years. The pointe shoe itself compresses the forefoot, and the mechanical demands of pointe work drive progressive angular deformity at the first metatarsophalangeal joint. Bunion formation, joint capsule thickening, and progressive articular cartilage loss in this joint create painful limitations that worsen after retirement when the protective conditioning of active training is lost.
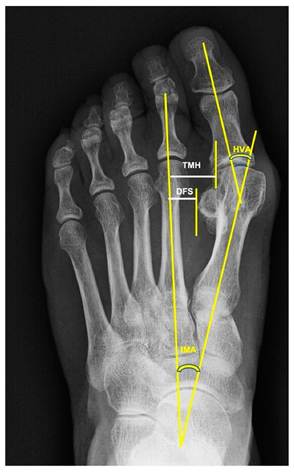
Hallux Valgus
Posterior impingement syndrome, caused by compression of soft tissue or an accessory os trigonum bone between the back of the tibia and the calcaneus during full plantarflexion, is another characteristically ballet-specific condition. Ankle instability from recurrent sprains, Achilles tendinopathy from the relentless demand placed on the calf complex, and stress fractures of the metatarsals and navicular round out a formidable inventory of foot pathology.

The Systemic Dimension: When Bone Density Becomes the Enemy
Underpinning many of these musculoskeletal injuries is a systemic vulnerability that the dance world has been slow to confront: the Female Athlete Triad. The combination of low energy availability driven by the aesthetic pressure to maintain extreme leanness, menstrual dysfunction, and diminished bone density creates a physiological environment in which bones are structurally compromised even as they are placed under extraordinary mechanical demand. Stress fractures, which might be merely inconvenient in an athlete with adequate bone density, become potentially career-ending events in dancers whose bones are prematurely osteopenic.
Research published in journals including the British Journal of Sports Medicine has documented lower bone mineral density in ballet dancers compared to age-matched controls, despite the weight-bearing nature of their activity, which would ordinarily be protective. The culprit is hormonal disruption from chronic energy restriction, which suppresses estrogen and impairs the osteoblastic activity needed to maintain bone density. The result is a dancer whose skeleton, despite extraordinary muscular development and technical mastery, is more fragile than it should be.
The Cultural Reckoning
What makes these injuries particularly poignant is their inevitability within the current structure of professional ballet. The training begins in childhood, typically between ages eight and twelve, when skeletal development is still incomplete and growth plates remain vulnerable. The aesthetic standards of the classical repertoire have changed little in a century. The pressure to perform through pain is embedded in the culture of most major companies, where taking a rest day can mean losing a role to a competitor waiting in the wings.

Misty Copeland’s willingness to document her surgical recovery publicly represents something genuinely new in this culture: the acknowledgment, by one of ballet’s most celebrated figures, that the body eventually presents its bill. Her recovery video is not an admission of weakness but an act of transparency — and perhaps an invitation for the art form to reckon honestly with what it costs its practitioners.

The grace that fills the stage at Lincoln Center or the Paris Opéra is real, but it is purchased at a price measured in labral tears and herniated discs, in bunioned feet and vertebral stress fractures, in joints worn decades beyond their years. Understanding that price is the first step toward demanding something better — better medical support, more honest conversations about physical limits, and an aesthetic evolution that might allow extraordinary artists to give more of their lives to their art.
— END —

Leave a comment