Taking Control of Your Biology
Biohacking sounds like something out of a sci-fi movie…implanting chips, editing genes, becoming superhuman. And while some of that exists on the extreme fringe, the reality is far more accessible and practical.
Biohacking is the practice of using science, technology, and self-experimentation to optimize your body and mind beyond their default settings.
Think of your body as hardware and your lifestyle as software. Most people run on the factory settings—whatever genetics, environment, and habit patterns installed by default. Biohackers refuse to accept these defaults. They ask: “What if I could upgrade my energy, cognitive performance, body composition, longevity, and overall quality of life through deliberate intervention?”
The Core Principle
At its heart, biohacking is about agency—taking active control rather than passive acceptance. It combines:
- Science: Understanding the biochemical, physiological, and neurological mechanisms that govern how your body functions
- Experimentation: Testing interventions on yourself and measuring results
- Optimization: Continuously refining your approach based on data and outcomes
This isn’t about following trends or quick fixes. It’s about understanding why something works (or doesn’t) at a mechanistic level, then applying that knowledge systematically.
The Spectrum of Biohacking
Biohacking exists on a spectrum from simple to extreme:
Foundational (Everyone Should Do This):
- Optimizing sleep quality and circadian rhythm
- Strategic nutrition timing and macronutrient ratios
- Resistance training and cardiovascular exercise
- Stress management and breathwork
- Supplement protocols (vitamin D, omega-3s, magnesium)
Intermediate (Data-Driven Optimization):
- Continuous glucose monitoring to personalize diet
- Wearable technology tracking (Oura Ring, WHOOP, Apple Watch)
- Cold and heat exposure (ice baths, sauna protocols)
- Intermittent fasting and metabolic flexibility training
- Nootropics (compounds that enhance cognitive function)
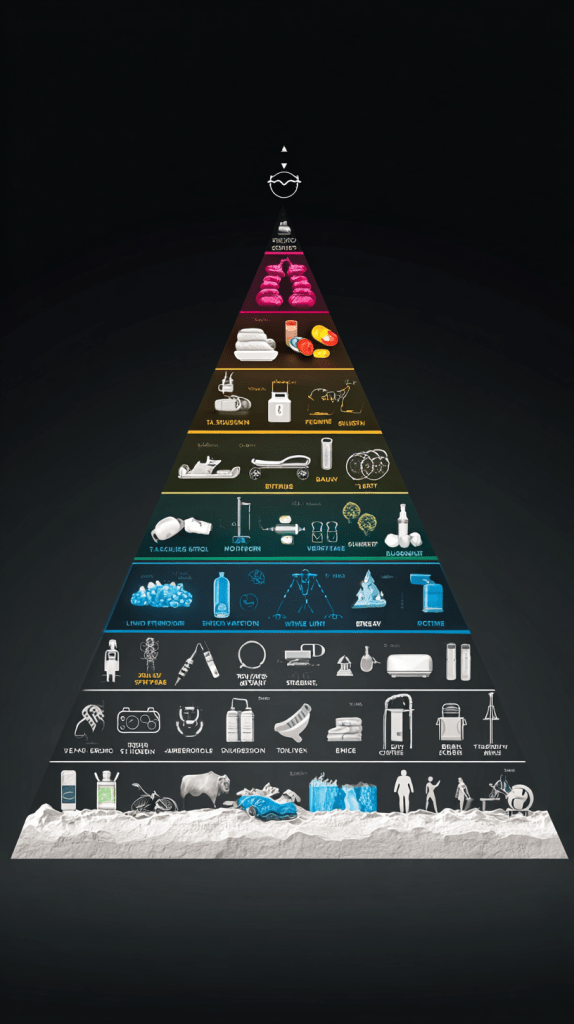
Advanced (Requires Medical Supervision):
- Peptide therapy (BPC-157, TB-500, growth hormone secretagogues)
- Hormone optimization (testosterone, thyroid, etc.)
- IV nutrient therapy and NAD+ infusions
- Photobiomodulation (red light therapy, near-infrared)
Extreme (Not for Most People):
- Implantable devices and chips
- Gene therapy and CRISPR applications
- Experimental longevity drugs (rapamycin, metformin, senolytics)
Why Biohack?
The modern environment is actively hostile to human health. We evolved for scarcity, movement, sunlight, and sleep—but we live in abundance, sitting, artificial light, and chronic stress. Our biology is mismatched with our environment.

Biohacking bridges that gap. It’s about:
- Reclaiming energy in a world designed to drain you
- Building resilience against environmental stressors
- Extending healthspan, not just lifespan (living longer well)
- Maximizing performance physically, mentally, and emotionally
The Biohacker’s Mindset
What separates biohackers from people just “trying to be healthy”?

1. Data over dogma: Biohackers measure. They track bloodwork, sleep metrics, body composition, cognitive performance. They don’t assume—they test and verify.
2. Mechanistic understanding: It’s not enough to know “vitamin D is good for you.” Biohackers understand how: it acts as a steroid hormone, regulating over 200 genes, modulating immune function, and influencing neurotransmitter synthesis.
3. Personalization: What works for one person may not work for another due to genetics, microbiome differences, and metabolic variability. Biohackers find their optimal protocol through experimentation.
4. Continuous iteration: Your body changes. Your needs change. Biohacking isn’t a destination—it’s an ongoing process of refinement.
The Bottom Line
Biohacking isn’t about perfection. It’s about optimization. It’s about refusing to settle for “fine” when “exceptional” is achievable through deliberate intervention.
You don’t need a lab, a medical degree, or unlimited resources to start. Begin with the fundamentals: fix your sleep, dial in your nutrition, move your body strategically, measure your progress.
Then, layer in more advanced protocols as you learn what your body responds to.
Your biology isn’t fixed. It’s malleable, adaptable, and waiting for you to take control.
The question isn’t whether you can biohack. The question is: why would you settle for anything less?