Uterine Fibroids, Black Women, and the Fight for Dignified Care
A Comprehensive Medical and Social Overview
Imagine living for years with crushing pelvic pain, hemorrhagic menstrual bleeding, and fatigue so severe it derails your career and relationships — only to be told by medical professionals that your symptoms are exaggerated, or that what you are experiencing is simply a part of being a woman. For countless Black women in the United States and around the world, this is not a hypothetical scenario. It is a lived reality, compounded by a well-documented history of medical bias that continues to shape clinical encounters today.
Uterine fibroids — noncancerous growths in or on the uterus — are extraordinarily common, yet they remain one of the most mismanaged and underappreciated conditions in women’s health. Nowhere is that mismanagement more consequential than in the care of Black women, who are disproportionately affected by fibroids in every measurable dimension: incidence, severity, age of onset, and symptom burden. Understanding why this disparity exists, and what must change to correct it, is not merely a medical question. It is a matter of justice.
“Black women are 2 to 3 times more likely to develop uterine fibroids than white women — and they develop them younger, larger, and in greater numbers.”
What Are Uterine Fibroids?
Uterine fibroids, known medically as uterine leiomyomas or myomas, are benign (noncancerous) tumors that arise from the smooth muscle cells of the uterine wall. They are composed primarily of smooth muscle tissue and fibrous connective tissue, which gives them their dense, rubbery consistency. Despite being labeled “tumors,” fibroids are not cancerous and have an extremely low rate of malignant transformation, estimated at less than 1 in 1,000 cases.
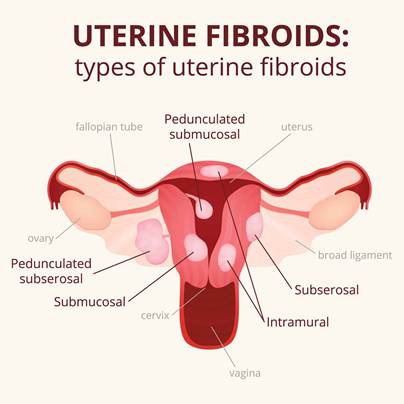
Fibroids are classified by their location within the uterus. Intramural fibroids, the most common type, grow within the muscular wall of the uterus. Subserosal fibroids develop on the outer surface of the uterus and can become pedunculated, growing on a stalk. Submucosal fibroids grow just beneath the inner lining of the uterus (the endometrium) and tend to cause the most significant bleeding symptoms. Cervical fibroids arise in the cervical tissue, and intraligamentary fibroids develop within the broad ligaments supporting the uterus.
Their size varies enormously from tiny seedlings detectable only under a microscope to massive growths that can distend the abdomen and weigh several pounds. A single woman may carry dozens of fibroids simultaneously, or just one. Their clinical impact depends heavily on size, number, and location.
Incidence: How Common Are Fibroids?
Uterine fibroids are the most common benign gynecologic tumor in women of reproductive age. By age 50, cumulative incidence studies suggest that up to 70% of white women and over 80% of Black women will have had fibroids, though many cases go undetected because a significant proportion of women remain asymptomatic.
In the United States alone, it is estimated that 26 million women between the ages of 15 and 50 have fibroids, with approximately 15 million experiencing symptoms severe enough to require treatment. Globally, fibroids account for roughly one-third of all hysterectomies performed — making them the leading cause of that procedure in the United States.
The Racial Disparity: Why Black Women Bear a Heavier Burden
The disparity between Black and white women in fibroid burden is among the starkest racial health disparities documented in the United States. Research consistently shows:
Black women are 2 to 3 times more likely than white women to develop fibroids. They develop fibroids at younger ages often in their 20s, compared to the 30s and 40s more typical of white women. Their fibroids tend to be larger and more numerous at the time of diagnosis. They experience more severe symptoms, including heavier menstrual bleeding, greater pelvic pain, and higher rates of anemia. They are more likely to require surgical intervention and undergo hysterectomy at higher rates and younger ages. They have a longer average delay between symptom onset and diagnosis — a gap often driven by dismissal from healthcare providers.
A landmark study published in the American Journal of Obstetrics and Gynecology found that by age 35, approximately 60% of Black women had ultrasound-confirmed fibroids, compared to 40% of white women. By age 50, those figures rose to over 80% and 70% respectively. Critically, the study also found that Black women’s fibroids were more likely to cause clinically significant symptoms.
Pathophysiology: The Biology Behind Fibroids
The development of uterine fibroids is a complex, multifactorial process involving genetic, hormonal, cellular, and environmental factors. While much remains to be fully elucidated, significant progress has been made in understanding the key mechanisms.
Hormonal Drivers
Estrogen and progesterone are the primary hormonal drivers of fibroid growth. Fibroids are rarely seen before puberty, grow during the reproductive years when hormone levels are highest, and typically shrink after menopause, a pattern that strongly implicates these hormones. Fibroids express higher concentrations of estrogen receptors and progesterone receptors compared to normal uterine tissue, and both hormones stimulate cell proliferation and suppress programmed cell death (apoptosis) within fibroid tissue.
Growth factors, including epidermal growth factor (EGF), transforming growth factor-beta (TGF-β), and insulin-like growth factors (IGFs), also appear to mediate the growth-promoting effects of estrogen and progesterone within fibroid tissue.
Genetic Mutations
Most fibroids are clonal in origin, meaning each tumor arises from a single transformed cell. Somatic mutations (acquired, not inherited) in the gene MED12 are found in the majority of fibroids, affecting up to 70% of cases. Other identified mutations involve HMGA2 (a chromatin-associated protein), FH (fumarate hydratase), and COL4A5/COL4A6 genes. These mutations disrupt normal cellular regulation, leading to unchecked proliferation and the overproduction of extracellular matrix proteins.
Race, Vitamin D, and Biological Stress
Researchers have explored several biological mechanisms that may explain the higher fibroid burden in Black women. One of the most compelling involves vitamin D. Black women have significantly higher rates of vitamin D deficiency due in part to increased skin melanin reducing ultraviolet light absorption, and vitamin D has been shown to inhibit fibroid cell proliferation in laboratory studies. Lower vitamin D levels may therefore remove a protective brake on fibroid growth.
Chronic stress related to racial discrimination, often termed “weathering” or allostatic load, is another important factor. Prolonged exposure to systemic racism elevates cortisol and inflammatory cytokine levels, alters hormonal regulation, and may create a biological environment more conducive to fibroid development and growth. This is not a reflection of biological inferiority; it is a biological consequence of living under conditions of chronic social and racial stress.
Additionally, studies have examined differences in hair relaxer use, dietary patterns, and environmental chemical exposures. Some research has found associations between hair relaxer chemicals (which may contain endocrine-disrupting compounds) and fibroid risk, though causation has not been definitively established.
“The higher fibroid burden in Black women is not a reflection of biological inferiority — it is, in substantial part, a consequence of the lived experience of racism itself.”
Clinical Presentation: Recognizing Symptoms
Approximately 25 to 50 percent of women with fibroids experience symptoms significant enough to affect their quality of life. The most common and debilitating symptoms include:
Heavy menstrual bleeding (menorrhagia) is the most reported symptom. Women may soak through pads or tampons within an hour, pass large blood clots, and experience bleeding that lasts for more than seven days. Severe blood loss can cause iron-deficiency anemia, leading to fatigue, shortness of breath, and heart palpitations. Pelvic pain and pressure, from a constant sense of heaviness to severe cramping, can be both cyclical and noncyclical. Dysmenorrhea (painful menstruation) may be debilitating. Bulk-related symptoms occur when large fibroids compress adjacent structures: urinary frequency and urgency arise from bladder compression; constipation and bloating from rectal compression; and back or leg pain from pelvic nerve pressure. Reproductive impact includes infertility, recurrent pregnancy loss, and obstetric complications including preterm labor and abnormal placentation. Abdominal distention caused by large fibroids may cause a woman to appear visibly pregnant.
Diagnosis: Getting to the Truth
Accurate and timely diagnosis is critical, and it is here that systemic bias begins to create divergent outcomes for Black women.
Diagnostic Tools
Pelvic ultrasound is the first-line diagnostic tool for fibroids. Transvaginal ultrasound provides the most detailed visualization of smaller or intramural fibroids. It is widely available, non-invasive, and cost-effective. Magnetic resonance imaging (MRI) provides superior anatomical detail, particularly important for surgical planning, and can more accurately map fibroid number, size, and location. Sonohysterography (saline-infused ultrasound) improves detection of submucosal fibroids by distending the uterine cavity with saline. Hysteroscopy allows direct visualization of the uterine interior and can be used both diagnostically and therapeutically for submucosal fibroids.
The Diagnostic Delay Problem
Despite the availability of these tools, Black women face substantially longer delays between the onset of symptoms and receiving a fibroid diagnosis. Studies have documented an average diagnostic delay of over three years for Black women, a span during which fibroids continue growing and symptoms worsen. This delay is not simply a matter of access to care, though access disparities are real and significant. It is also a product of implicit bias, paternalism, and the systematic discounting of Black women’s pain.
Research has consistently shown that healthcare providers are less likely to prescribe adequate pain management to Black patients, more likely to attribute their symptoms to psychological causes, and more likely to dismiss their concerns without appropriate investigation. The result is that women who should be receiving pelvic ultrasounds are instead being told their pain is stress-related, that their bleeding is “normal,” or that they simply need to lose weight.
Prognosis: Living With Fibroids
Fibroids are not life-threatening, but their impact on quality of life can be profound. Women with symptomatic fibroids report significantly impaired physical functioning, social limitations, and emotional wellbeing. Work productivity losses due to heavy bleeding and pain, including missed workdays and reduced effectiveness,cost an estimated $4,000 to $6,000 per woman per year in the United States.
Most fibroids remain stable or grow slowly. After menopause, the majority shrink as estrogen levels decline. However, for women still in their reproductive years, the condition is often progressive without treatment. Untreated iron deficiency anemia from chronic blood loss can cause serious cardiovascular strain. Submucosal fibroids significantly reduce fertility and implantation rates. Pregnancy complications, including preterm delivery and placental abruption, are elevated in women with fibroids, particularly larger ones.
The prognosis following appropriate treatment is generally excellent, with most women experiencing substantial or complete symptom relief. The key word is “appropriate” which requires both access to care and providers who listen.
Treatment Options: A Spectrum of Possibilities
Fibroid treatment has expanded considerably in recent decades, offering women options ranging from watchful waiting to minimally invasive procedures to surgery. The ideal treatment depends on symptom severity, fibroid characteristics, reproductive goals, and patient preference, and every woman deserves a thorough, individualized conversation about her options.
Medical (Non-Surgical) Treatments
Hormonal therapies including combined oral contraceptives, progestin-only agents, and levonorgestrel-releasing intrauterine devices (IUDs) can reduce menstrual bleeding and relieve pain, though they do not shrink fibroids. GnRH agonists (gonadotropin-releasing hormone agonists) such as leuprolide suppress ovarian hormone production, causing fibroids to shrink temporarily. They are often used preoperatively to reduce fibroid size and blood loss but are not suitable for long-term use due to side effects including bone loss and menopausal symptoms. GnRH antagonists, including elagolix (Oriahnn) and relugolix (Myfembree), offer a newer approach with more rapid onset and some advantages in tolerability. They are now FDA-approved for fibroid-associated heavy menstrual bleeding. Tranexamic acid is a non-hormonal medication that reduces menstrual blood loss by stabilizing blood clots and can significantly reduce bleeding volume. Iron supplementation addresses anemia caused by chronic blood loss and is an important supportive therapy.
Minimally Invasive Procedures
Uterine fibroid embolization (UFE) is a radiological procedure in which the blood supply to fibroids is blocked by injecting small particles through a catheter inserted into the uterine arteries. Fibroids shrink significantly over months, with sustained symptom relief in approximately 85 to 90 percent of women. UFE preserves the uterus and has a shorter recovery time than surgery, though it is not typically recommended for women desiring future pregnancy. Focused ultrasound ablation uses high-intensity ultrasound waves, guided by MRI, to heat and destroy fibroid tissue. It is completely non-invasive and preserves fertility. Endometrial ablation destroys the uterine lining and can dramatically reduce bleeding, but it is only appropriate for women who do not wish to conceive and is best suited for smaller, submucosal fibroids.
Surgical Treatments

Myomectomy is the surgical removal of fibroids while preserving the uterus. It can be performed via hysteroscopy (for submucosal fibroids), laparoscopy, robotic assistance, or open abdominal surgery depending on fibroid size and location. Myomectomy is the preferred surgical option for women who wish to preserve fertility. Hysterectomy, complete removal of the uterus, is the only definitive cure for fibroids. It eliminates any possibility of fibroid recurrence and resolves all associated symptoms permanently. However, it also permanently ends fertility and carries surgical risks. Hysterectomy remains disproportionately performed in Black women with fibroids, a disparity reflecting both the greater severity of their disease at presentation and, in some cases, inadequate counseling about uterus-sparing alternatives.
“Every woman deserves a thorough, individualized conversation about her treatment options — not an assumption that hysterectomy is her only choice.”

The Medical Bias Crisis: When Pain Is Dismissed
The undertreatment of Black women’s pain is not a new phenomenon ; it is a pattern with deep historical roots and ongoing contemporary consequences. The myth that Black people have higher pain thresholds, or that their reported pain is exaggerated, has been traced to 19th-century pseudoscientific claims made by physicians who used enslaved Black bodies as medical subjects without anesthesia. These racist ideologies were never fully eradicated from medical culture; they evolved and persisted, embedded in implicit bias that continues to shape clinical decisions.
A widely cited 2016 study published in the Proceedings of the National Academy of Sciences found that medical students and residents — even those without overt prejudice — were significantly more likely to hold false beliefs about biological differences between Black and white patients (such as Black people having thicker skin or less sensitive nerve endings) and that those who held such beliefs were less likely to recommend adequate pain treatment for Black patients. This is not anecdote. It is published, peer-reviewed science demonstrating that bias translates into undertreatment.
For Black women with fibroids, this manifests in concrete, harmful ways. Their heavy bleeding is attributed to lifestyle. Their pelvic pain is called stress. Their requests for imaging are denied. Their descriptions of disability are questioned. And when they finally do receive a diagnosis, they are often offered only the most extreme intervention — hysterectomy — rather than being counseled about the full range of options their white counterparts routinely receive.
What Must Change: Building Equitable, Dignified Care
Providing equitable, dignified care to Black women with fibroids requires change at every level of the healthcare system — individual, institutional, and structural. The following evidence-based and justice-centered recommendations represent a roadmap for meaningful reform.
1. Believe Women — Unconditionally
The foundation of dignified care is the radical but simple act of believing patients. When a woman reports pain, bleeding, or functional impairment, the clinical response should be investigation, not skepticism. Pain should be documented, taken seriously, and evaluated with appropriate tools, not minimized because of assumptions rooted in race, size, or social status. Every provider must actively examine and challenge their assumptions about which patients’ reports of suffering are credible.
2. Eliminate Implicit Bias Through Training and Accountability
Medical schools, residency programs, and continuing medical education must integrate robust, evidence-based implicit bias training into their curricula. But training alone is insufficient. Hospitals and practices must implement accountability structures — tracking prescribing patterns, referral rates, and diagnostic delays by patient race and use that data to identify and address disparities. What gets measured gets managed.
3. Standardize Early Screening for High-Risk Populations
Given the earlier onset and greater severity of fibroids in Black women, professional medical societies should develop and implement screening guidelines that specifically address this population. A Black woman who presents to a primary care physician or gynecologist with heavy menstrual bleeding or pelvic pain should receive a pelvic ultrasound, period. Delays in diagnostic imaging must be treated as a quality-of-care failure, not an acceptable norm.
4. Expand Access to Uterus-Preserving Treatments
Black women are significantly more likely to end up with a hysterectomy than white women with comparable fibroid burden — not because their medical situation necessarily requires it, but because they are less frequently counseled about alternatives and less frequently referred to specialists who perform them. Providers must commit to presenting the full spectrum of treatment options, and healthcare systems must ensure that procedures like UFE, focused ultrasound, and laparoscopic myomectomy are accessible regardless of a patient’s insurance status or zip code.
5. Center Patient Autonomy and Reproductive Goals
Treatment decisions must be driven by the patient’s goals, values, and reproductive desires — not by assumptions based on race or socioeconomic status. A Black woman who wants to preserve her fertility and uterus has every right to pursue treatments that honor that goal. A Black woman who chooses hysterectomy for her own reasons has every right to that decision as well. The difference is whether the choice is hers, made with full information, versus a decision made for her without adequate counseling.
6. Invest in Research That Centers Black Women
Historically, fibroid research has underrepresented Black women despite their greater disease burden. NIH funding must be prioritized for studies that examine fibroid etiology in Black women specifically, assess the effectiveness of different treatments in Black patients, and investigate the role of social determinants — including discrimination, chronic stress, and environmental exposures — in fibroid development. The disparities cannot be understood or addressed without data that reflects them.
7. Diversify the Medical Workforce
Research consistently shows that Black patients receive better care from Black physicians — not merely because of cultural concordance, but because of different patterns of listening, communication, and clinical attention to patient-reported symptoms. Increasing the representation of Black physicians, nurses, and other healthcare professionals — particularly in obstetrics and gynecology — is both a workforce equity imperative and a patient safety strategy.
8. Empower Patients Through Education and Advocacy
Black women must be equipped with knowledge about fibroids — their symptoms, their options, and their rights as patients. Community health organizations, patient advocacy groups such as the White Dress Project, and social media platforms have already begun this work, helping women name their symptoms, document their experiences, and demand appropriate care. Healthcare systems should partner with — not co-opt — these community voices. Patients who arrive armed with information and the confidence to advocate for themselves are more likely to receive the care they deserve.
9. Reform Clinical Communication Standards
Provider-patient communication must be assessed and reformed. Scripts that embed dismissal — “some women just bleed more heavily,” “your pain tolerance might be lower,” “let’s watch and wait” without clinical justification — must be recognized for what they are: clinical failures with racial dimensions. Medical education must teach providers to communicate with humility, to invite patients’ perspectives, and to avoid language that diminishes or invalidates reported symptoms.
Conclusion: The Moral Urgency of Getting This Right
Uterine fibroids are not a mystery. We understand their biology, we have effective treatments, and we know who suffers most. What we lack is not knowledge ; it is the will to apply that knowledge equitably.
Black women in America have long been required to prove that their pain is real, that their suffering matters, and that they deserve the same standard of care as anyone else. That requirement is itself a form of harm layered on top of the physical burden of a condition that already disproportionately claims their energy, their fertility, and in severe cases, their organs.
Changing this will not happen through goodwill alone. It requires structural change in medical education, in research funding, in clinical protocols, and in the culture of medicine itself. It requires every provider who sees a Black woman in pain to ask themselves a simple question: Would I respond the same way if this patient were white?
Until the answer to that question is always “yes” — and the evidence confirms it — the work is not done.
“Black women deserve to be believed. They deserve to be heard. They deserve to receive the same quality of care on the first appointment that it may take others years and multiple providers to obtain.”
This article is intended for educational purposes. Women experiencing gynecologic symptoms should seek care from a qualified healthcare provider. If you feel your concerns are being dismissed, you have the right to seek a second opinion.

Leave a comment