The Dangerous Truth Behind Bodybuilding’s Shortcut
A medical and scientific examination of a dangerous practice
In gyms and online forums dedicated to extreme bodybuilding, a substance called synthol has circulated for decades, promising what years of training cannot deliver: instant, dramatic muscle size. What is rarely discussed with equal candor are the consequences, including abscesses that require surgical drainage, oil emboli that can kill, limbs lost to amputation, and the silent, irreversible destruction of muscle tissue at the cellular level. This article examines synthol with the seriousness the subject demands.

What Is Synthol?
Synthol is not an anabolic steroid, though it is often grouped with performance-enhancing substances in discussions of bodybuilding doping. It was developed in the early 1990s by German gym owner Chris Clark, who originally marketed it under the name “Pump N’ Pose” as a posing oil, a cosmetic product for competitive bodybuilders to apply to the skin. The formulation was designed specifically to be injected directly into muscle tissue.
The standard composition of synthol is approximately 85% medium-chain triglyceride (MCT) oil, typically caprylic/capric triglycerides derived from coconut or palm oil — combined with roughly 7.5% lidocaine, a local anesthetic, and 7.5% benzyl alcohol, which acts as a preservative and solubilizer. Some formulations sold through underground channels vary these proportions or substitute alternative oils, increasing unpredictability and risk.
Synthol is classified as a “site enhancement oil” (SEO). It is not approved by any regulatory body, including the U.S. Food and Drug Administration, for injection into human tissue. It is sold in some countries as a “posing oil” to circumvent legal restrictions, with the understanding among buyers that it will be injected.
Why People Inject It
The appeal of synthol is straightforward: it creates the appearance of larger muscles almost immediately. When injected into a muscle belly, the oil physically distends the fascial compartments within the muscle, producing visible swelling that mimics hypertrophy. For competitive bodybuilders seeking to fill in a lagging muscle group days before a contest, or for individuals who want a shortcut to an imposing physique, synthol offers a rapid, if deeply deceptive, solution.
Psychologically, the practice is often rooted in body dysmorphia, a condition in which individuals perceive their bodies as inadequate despite objective evidence to the contrary. The bodybuilding and fitness communities that celebrate extreme muscularity can amplify these perceptions, and social media has broadened the audience for extreme physiques, creating demand and a degree of social validation for dangerous self-modification.
Some users also report using synthol to correct asymmetries — attempting to balance a bicep or calf that appears smaller than its counterpart. The promise of a targeted, controllable fix is seductive, particularly when the alternative is years of additional training that may never fully resolve the disproportion.
How It Is Injected
The injection protocols described in underground bodybuilding communities are elaborate and reflect a troubling pseudo-medical sophistication. Users typically inject synthol into the belly of a target muscle using a syringe with a needle long enough to penetrate the muscular fascia, commonly 23 to 25 gauge needles, one to one and a half inches in length.
Volumes injected vary, but protocols described online often begin with 1 mL per injection site and escalate over weeks to 3 mL or more per site, with multiple injection points per muscle to attempt an even distribution of oil. For biceps, for example, injections may be made at several depths along the muscle belly. The cumulative volume introduced into a single muscle over a “cycle” can reach 10 to 30 mL or more.
The lidocaine component serves a practical purpose: it blunts the pain of injection, making higher volumes more tolerable and allowing users to continue the practice despite warning signs their bodies are producing. This analgesic effect is itself dangerous, as pain is a critical physiological signal that injection is causing tissue damage.
These injections are almost universally self-administered, without sterile technique, without imaging guidance, and without any formal medical knowledge of local anatomy. The proximity of major blood vessels, nerves, and joint structures to common injection sites makes blind needle placement particularly hazardous.
Medical Complications: What Synthol Actually Does
Embolism
Perhaps the most immediately life-threatening complication of synthol injection is oil embolism, the entry of oil droplets into the bloodstream. When a needle inadvertently punctures a vein or artery, or when oil migrates through damaged tissue into the vasculature, droplets can be carried through the circulatory system to the lungs, heart, or brain.
Pulmonary oil embolism, the obstruction of pulmonary vessels by oil, presents with acute respiratory distress, pleuritic chest pain, hypoxia, and can progress to cardiovascular collapse and death. The condition is notoriously difficult to diagnose quickly because imaging findings may be subtle, and the treating team may not be aware that the patient has been injecting oil into their muscles. Case reports in the medical literature document patients who presented to emergency departments in respiratory failure with no prior cardiac history, only for autopsy or CT imaging to reveal extensive oil deposition in the pulmonary vasculature.
Stroke resulting from cerebral oil embolism has also been documented in synthol users, with oil droplets traveling through cardiac shunts or other pathways to obstruct cerebral vasculature. These events can result in permanent neurological deficits or death.
Infections and Abscesses
Non-sterile injection technique in an oil-rich tissue environment creates ideal conditions for bacterial infection. The lipid content of synthol acts as an excellent growth medium for bacteria, and the disrupted tissue architecture impairs the normal immune surveillance that would otherwise contain an early infection.
Abscesses, loculated collections of pus within the muscle, are among the most commonly reported complications. They can grow to enormous size within the confines of the muscular fascia before becoming clinically apparent, in part because the overlying skin may appear relatively normal and because the lidocaine component of synthol suppresses pain. When these abscesses are finally recognized, they frequently require surgical incision and drainage, debridement of necrotic tissue, and prolonged courses of intravenous antibiotics.

Cases of necrotizing fasciitis, a rapidly spreading, life-threatening soft tissue infection, have been reported following synthol injections. In this condition, bacterial infection spreads along fascial planes, destroying tissue faster than the immune system can respond. Treatment requires emergency surgery with aggressive removal of all infected tissue; mortality rates are high even with optimal care.

Muscle Fibrosis
Even in the absence of dramatic acute complications, the chronic introduction of oil into muscle tissue causes progressive, irreversible fibrosis. The body recognizes foreign oil as an irritant and mounts an inflammatory response — but because the oil is not efficiently metabolized or cleared, this response becomes chronic.

White fibers signifying Muscle fibrosis seen via CT Scan
Over time, the inflammatory infiltrate gives way to fibroblast activation and collagen deposition. The functional muscle tissue is gradually replaced by scar tissue, dense, inelastic fibrous material that neither contracts nor generates force. The muscle may appear visually larger due to the oil and fibrotic deposits, but it becomes progressively weaker and less functional. This process is largely irreversible; unlike true hypertrophy, fibrosis cannot be trained away.
Effects on Muscle Biology at the Cellular Level
To understand what synthol does to muscle tissue, it is important to appreciate the architecture of healthy skeletal muscle. Muscle fibers, individual multinucleated cells called myocytes, are organized into bundles called fascicles, each wrapped in connective tissue. The functional units within each fiber are sarcomeres, repeating structures of actin and myosin filaments whose synchronized contraction generates force. The entire structure is densely vascularized and innervated.
When oil is injected into this environment, it initially occupies the spaces between fascicles and between individual muscle fibers. The oil is not water-soluble, so it cannot be absorbed into the aqueous interstitial fluid or cleared through normal lymphatic drainage efficiently. Instead, it persists as discrete oil droplets and larger oil lakes within the tissue.
At the cellular level, the body’s response begins with macrophage infiltration. Macrophages — the immune system’s primary tissue-resident scavengers — attempt to phagocytose the oil droplets, becoming lipid-laden “foam cells” identical in appearance to those seen in atherosclerotic plaques. These foam cells aggregate into granulomas — organized clusters of immune cells attempting to wall off material they cannot destroy.
The sustained presence of oil and the chronic inflammatory response it provokes disrupts satellite cell function. Satellite cells — the stem cell population responsible for muscle repair and growth — reside in a niche between the muscle fiber membrane and the basement membrane. Chronic inflammation alters the signaling environment these cells depend on for activation and differentiation, impairing the muscle’s normal capacity for repair and adaptation.
Transforming growth factor-beta (TGF-β), a cytokine released in large quantities during chronic inflammation, drives fibroblast activation and collagen synthesis — the cellular basis of fibrosis. As collagen accumulates within the endomysium and perimysium (the connective tissue layers surrounding individual fibers and fascicles), it mechanically compresses viable muscle fibers, impairing their blood supply and innervation. Myocytes deprived of adequate oxygen and neurotrophic signaling undergo atrophy and eventually apoptotic or necrotic cell death.
Histological examination of biopsies from synthol-injected muscle, described in several case reports, reveals a striking and sobering picture: what was once organized, functional muscle tissue has been transformed into an admixture of oil vacuoles, inflammatory cells, fibrous tissue, and remnant muscle fibers in varying states of degeneration. The tissue resembles a pathological specimen from chronic inflammatory myopathy more than it does healthy skeletal muscle.
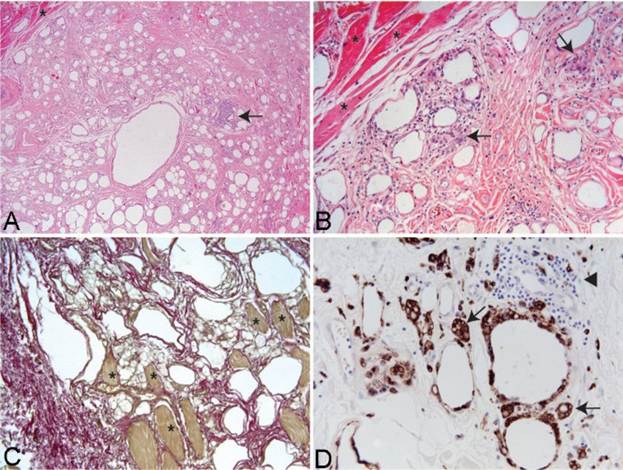
Microscopy of tissue sections of muscle injected with Synthol causing chronic pain
When Surgery — and Amputation — Becomes Necessary
The surgical consequences of synthol use exist on a spectrum from drainage procedures to limb amputation, and the path from one end to the other can be disturbingly short.
In milder cases, the accumulation of oil and abscess formation requires surgical incision and drainage. Surgeons describe encountering large volumes of liquefied oil and pus, sometimes hundreds of milliliters, within muscle compartments during these procedures. Multiple surgeries are often required, and the wound must be managed carefully to prevent re-infection of the compromised tissue.

Abscess drainage
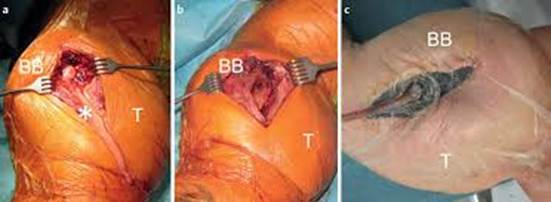
In more severe cases, the combination of infection, vascular compromise, and tissue necrosis may render a limb unsalvageable. When blood supply to a limb is critically compromised — whether through direct vascular injury, compartment syndrome, or widespread tissue destruction — amputation may become the only option to save the patient’s life. Several case reports in the medical literature document patients who underwent arm or leg amputation as a direct consequence of complications arising from site enhancement oil injections.

Prelude to amputation
Even in cases that do not progress to amputation, the functional outcomes of surgery are often poor. Removal of oil-infiltrated, fibrotic tissue inevitably removes functional muscle as well, leaving patients with significant weakness and deformity. The cosmetic result, often the original motivation, is typically worse after surgery than it was before synthol was ever injected.
grey necrotic muscle developing after Synthol injection
Notable Cases and Fatalities
The medical literature on synthol-related deaths is limited, in part because cause of death is not always linked to synthol use in official records, and because many users do not disclose their injection practices to treating physicians. Nonetheless, documented cases paint a clear picture of a lethal potential.
Case reports published in journals including the Journal of Forensic Sciences and various emergency medicine publications describe deaths attributed to pulmonary oil embolism in individuals found post-mortem to have injected site enhancement oils. In one autopsy series, oil droplets were identified throughout the pulmonary microvasculature in a young male who died suddenly; interview with family members subsequently revealed a pattern of intramuscular oil injection.
Perhaps the most widely publicized cases involve Brazilian bodybuilder Arlindo de Souza, known in media coverage as the “Mountain Man,” who injected synthol and other substances into his arms, developing biceps reportedly measuring 29 inches in circumference. While he survived initially, physicians who examined him warned that the oil had severely compromised the vascularity and function of his arm muscles, and that he faced a high risk of amputation. He died at age 55.
Arlindo de Souza
Brazilian bodybuilder Romario Dos Santos Alves became another prominent cautionary case after years of synthol and alcohol injection into his arms left him with massively deformed limbs, severe chronic pain, and arms described by treating surgeons as having the consistency of rock — the oil had calcified within the fibrotic tissue. He narrowly avoided bilateral arm amputation; surgeons were only able to prevent it by performing extensive debridement procedures.

Romario dos Santos Alves
Beyond individual cases that reached media attention, emergency departments in countries where bodybuilding subcultures are prominent report a steady stream of patients presenting with synthol-related complications — infections, abscesses, respiratory distress — many of whom initially deny having injected anything. The true burden of synthol-related morbidity and mortality is almost certainly underreported.
A Substance Without a Safe Use
Unlike anabolic steroids, which are pharmaceutical compounds with genuine medical applications and a body of research quantifying their risks, synthol has no legitimate therapeutic use. It is a foreign oil injected into one of the body’s most metabolically active tissues, without any mechanism for safe elimination, and with a well-documented capacity to cause permanent damage, serious infection, life-threatening embolism, and death.
The appearance synthol creates is not muscle. It is oil trapped in a tissue it is destroying. The muscle that users are trying to enlarge becomes progressively less capable of the function it evolved to perform, movement, force generation, and the physical expression of genuine fitness.
For those in medical practice, awareness of synthol and site enhancement oils is clinically important. Patients presenting with unusual soft tissue swelling, recurrent abscesses, unexplained respiratory distress, or stroke in young men with extreme physiques should prompt consideration of intramuscular oil injection in the differential. Establishing this history requires a non-judgmental approach; many patients are reluctant to disclose the practice due to shame or fear of legal consequences.
For those considering synthol, or those who know someone who is: the consequences described in this article are not hypothetical worst cases. They are documented outcomes that occur with regularity. There is no safe dose, no safe protocol, and no version of this practice that does not carry the risk of permanent harm or death.This article is intended for educational and informational purposes. If you or someone you know is struggling with body image, disordered exercise behavior, or the use of performance-enhancing substances, please seek support from a qualified medical or mental hhealth professional.

Leave a comment