Whether you’re a skincare enthusiast, a biohacker optimizing your body from the outside in, or someone living with one of these conditions — this guide is for you. Skin is your largest organ, your first line of immune defense, and, frankly, a mirror of everything happening inside. Let’s get into it.
- Hyperpigmentation

Hyperpigmentation is one of the most widespread skin concerns globally, affecting people of all skin tones — though it’s significantly more common and visible in deeper skin tones. It occurs when excess melanin (the pigment responsible for skin color) deposits in patches, creating areas darker than the surrounding skin.
Causes: UV exposure, hormonal shifts, inflammation, certain medications (like antimalarials or chemotherapy drugs), and metabolic conditions. Sun exposure is both a primary cause and an accelerant of existing pigmentation.
Diagnosis: Usually clinical (a dermatologist can identify it by sight), sometimes aided by a Wood’s lamp or dermoscopy.
Treatment: This is where it gets exciting for biohackers. Topical agents like vitamin C, niacinamide, kojic acid, azelaic acid, retinoids, and hydroquinone (the gold standard) are first-line. Chemical peels (glycolic, lactic, TCA), laser therapy (Q-switched Nd:YAG, fractional CO2), and intense pulsed light (IPL) can deliver dramatic results. Consistent broad-spectrum SPF 30+ is non-negotiable — without it, every treatment is fighting uphill.
Cure: Manageable and often reversible, but not always permanently “cured” — prevention and maintenance are key.
2. Post-Inflammatory Hyperpigmentation (PIH)

PIH is hyperpigmentation’s close cousin — the dark marks left behind after skin trauma. Acne, burns, cuts, eczema flares, or any wound can trigger melanocytes to overproduce pigment during the healing process.
How common: Extremely common, particularly in Fitzpatrick skin types IV–VI (brown to dark skin), where it can be more distressing than the original condition.
Causes: Any inflammatory insult to the skin. The inflammation signals melanocytes to ramp up melanin production as a protective response.
Diagnosis: Clinical, based on history and appearance.
Treatment: Same arsenal as hyperpigmentation — retinoids, vitamin C, niacinamide, azelaic acid, chemical exfoliants. Time is also a healer (superficial PIH fades in months; deep dermal PIH can take years). Lasers must be used cautiously in darker skin tones to avoid worsening pigmentation.
3. Melasma

Melasma is the “mask of pregnancy” — symmetrical brown-gray patches typically appearing on the cheeks, forehead, upper lip, and chin. It affects an estimated 5–6 million people in the U.S. alone, with women making up about 90% of cases.
Causes: A perfect storm of UV exposure, hormonal influence (estrogen, progesterone), and genetic predisposition. Oral contraceptives and pregnancy are classic triggers.
Diagnosis: Clinical. Dermoscopy and Wood’s lamp help assess the depth (epidermal vs. dermal vs. mixed).
Treatment: The Kligman formula (hydroquinone + tretinoin + corticosteroid) remains a time-tested combination. Tranexamic acid (oral and topical) has emerged as a game-changer. Chemical peels and laser (used carefully) can help. The frustrating truth: melasma is chronic and recurrence is common, especially without aggressive sun protection.
Cure: Controlled, not cured. Think of it as a managed condition.
4. Rosacea

Rosacea is a chronic inflammatory skin condition affecting over 16 million Americans, characterized by facial redness, visible blood vessels, and sometimes acne-like pustules. It most commonly affects fair-skinned adults between 30–60.
Causes: The exact mechanism isn’t fully understood, but contributors include Demodex mite overpopulation, dysregulation of the innate immune system, neurovascular dysfunction, and gut microbiome imbalances (rosacea is strongly associated with small intestinal bacterial overgrowth/SIBO).
Subtypes: Erythematotelangiectatic (redness-dominant), papulopustular (acne-like), phymatous (skin thickening, often around the nose), and ocular.
Diagnosis: Clinical, based on characteristic presentation.
Treatment: Topical metronidazole, azelaic acid, ivermectin (Soolantra), and brimonidine for redness. Oral doxycycline (low-dose) for inflammatory subtypes. Laser and IPL for vascular components. Biohackers take note: dietary triggers (alcohol, spicy food, heat) are highly individual — an elimination approach combined with a food diary can be revealing. Gut health optimization is an underexplored avenue.
5. Stretch Marks (Striae)

Stretch marks affect roughly 70% of adolescent girls, 40% of boys, and up to 90% of pregnant women — making them one of the most common skin findings on the planet, yet one of the most emotionally loaded.
Causes: Rapid stretching of skin during growth spurts, pregnancy, rapid weight gain or loss, or bodybuilding. Corticosteroid use (topical or systemic) is another major driver. When the dermis tears, collagen and elastin fibers rupture.
Types: Striae rubrae (red, active) and striae albae (white, mature). Red striae are easier to treat.
Diagnosis: Visual.
Treatment: Tretinoin creams have the best evidence for early (red) stretch marks. Microneedling, radiofrequency, fractional laser (especially CO2 or Fraxel), and platelet-rich plasma (PRP) have all shown promising results. No treatment fully erases mature white stretch marks, but significant improvement is achievable.
6. Acne (Pubescent & Adult)

Acne is the world’s most common skin condition, affecting approximately 85% of people between 12–24 at some point, and increasingly persistent into adulthood (adult acne affects up to 15% of women and 5% of men over 25).
Causes: The four horsemen of acne: excess sebum production, follicular hyperkeratinization, Cutibacterium acnes (formerly P. acnes) bacterial overgrowth, and inflammation. Hormonal fluctuations, high-glycemic diets, dairy consumption, stress, and certain medications (steroids, lithium) are recognized amplifiers.

Diagnosis: Clinical grading (comedonal, papulopustular, nodulocystic).
Treatment: Mild: benzoyl peroxide, salicylic acid, retinoids, niacinamide. Moderate: topical or oral antibiotics, combined with retinoids. Severe/cystic: isotretinoin (Accutane) remains the only treatment approaching a cure. Hormonal therapy (spironolactone, OCP) is effective in women with hormonal-pattern acne. For biohackers: eliminating high-glycemic foods and dairy has meaningful evidence behind it. Gut microbiome health and zinc levels are worth investigating.
Adult acne note: Often driven differently than teen acne — stress hormones, hormonal fluctuations, and inflammatory diets play a larger role.
7. Hair Loss: Male Pattern Baldness, Female Hair Loss & Alopecia

Hair loss is deeply personal. Androgenetic alopecia (pattern baldness) affects roughly 50 million men and 30 million women in the U.S. But the umbrella of alopecia is wide.
Male Pattern Baldness (Androgenetic Alopecia): Driven by DHT (dihydrotestosterone) shrinking hair follicles over time. Hereditary. Follows the Hamilton-Norwood scale.
Female Hair Loss: Often more diffuse. PCOS, thyroid dysfunction, iron deficiency, and hormonal shifts (postpartum, perimenopause) are frequent culprits alongside genetics.
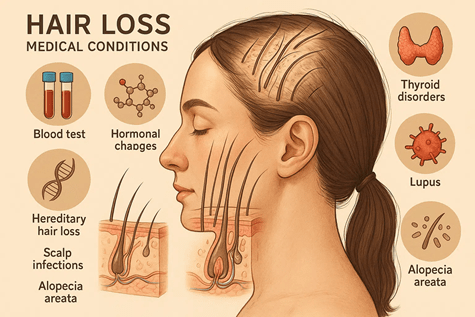
Alopecia Areata: An autoimmune condition where the immune system attacks hair follicles, causing patchy loss. Can progress to alopecia totalis (entire scalp) or universalis (entire body). Affects ~2% of people globally.
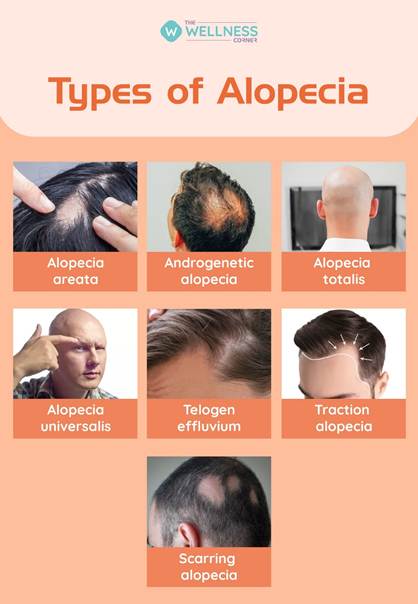
Traction Alopecia: Caused by persistent mechanical tension from hairstyles.
Telogen Effluvium: Diffuse shedding triggered by physical or emotional shock (illness, surgery, crash dieting, trauma).
Diagnosis: Trichoscopy, pull test, scalp biopsy, blood panels (thyroid, iron, androgens, ANA).
Treatment: Minoxidil (topical or oral) is first-line for most types. Finasteride/dutasteride for men (and select women). JAK inhibitors (baricitinib, ritlecitinib) represent a breakthrough for alopecia areata — ritlecitinib received FDA approval in 2023. PRP, low-level laser therapy (LLLT), and hair transplantation round out the options. Biohackers often investigate iron optimization, ashwagandha, saw palmetto, and scalp microneedling with minoxidil synergistically.
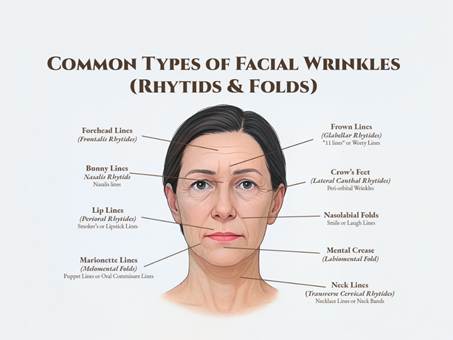
8. Rhytids (Wrinkles)

Wrinkles are the skin’s autobiography — written in sun exposure, expressions, sleep habits, and the passage of time. They’re universal but vary dramatically based on genetics, lifestyle, and skin care.
Types: Dynamic rhytids (from muscle movement — crow’s feet, forehead lines) and static rhytids (visible at rest, from collagen/elastin loss and photodamage).
Causes: UV-induced collagen degradation, reduced hyaluronic acid production, glycation, inflammation, smoking, and repeated facial movement.
Treatment: Retinoids (tretinoin) are the gold standard topical — they genuinely stimulate collagen. Antioxidants (vitamin C, resveratrol, niacinamide) help slow degradation. Botulinum toxin (Botox, Dysport) for dynamic lines. Dermal fillers (hyaluronic acid, calcium hydroxylapatite) for static lines and volume loss. Fractional laser, microneedling with RF, ultrasound (Ultherapy), and chemical peels for skin resurfacing. For biohackers: collagen peptide supplementation, glycation management (low-sugar diets), red light therapy, and sleep optimization all have evidence-backed merit.
9. Vitiligo

Vitiligo is striking — patches of skin lose all pigment, creating stark white areas against surrounding skin. It affects approximately 1–2% of the global population across all skin types, though it’s most visible in darker skin.
Causes: Autoimmune destruction of melanocytes. Genetic predisposition interacts with environmental triggers. Associated with other autoimmune conditions (thyroid disease, type 1 diabetes, rheumatoid arthritis).
Diagnosis: Clinical. Wood’s lamp illuminates depigmented patches vividly. Biopsy confirms absence of melanocytes.
Treatment: Topical corticosteroids, calcineurin inhibitors (tacrolimus). Narrowband UVB phototherapy is highly effective. The game-changer: ruxolitinib (Opzelura) cream — a JAK inhibitor — received FDA approval in 2022 specifically for vitiligo, the first targeted therapy for the condition. Oral and topical JAK inhibitors are reshaping the treatment landscape. Repigmentation can be remarkable with treatment.
10. Skin Infections
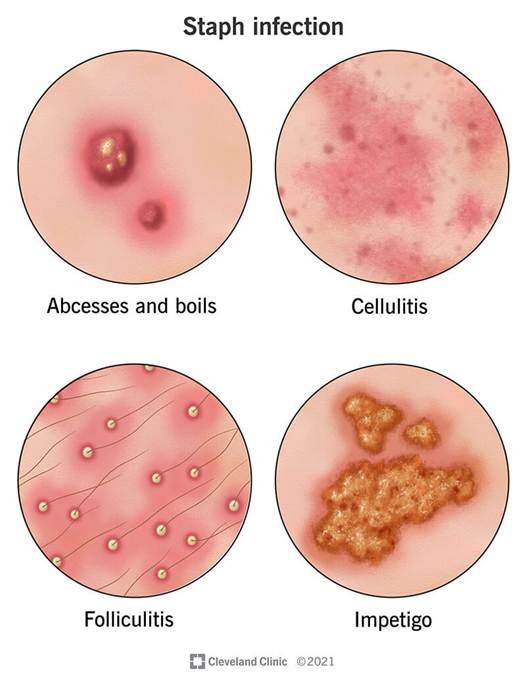
Skin is a battlefield, and sometimes the microbes win.
Impetigo: Highly contagious superficial bacterial infection (usually S. aureus or Strep pyogenes), common in children. Golden-crusted lesions around the nose and mouth. Treated with topical mupirocin or oral antibiotics.
Erysipelas: A bright red, well-demarcated, warm superficial skin infection — classically affecting the face or lower legs. Almost always caused by Group A Streptococcus. IV or oral penicillin is curative.
Staph Infections (MRSA and MSSA): Staphylococcus aureus is a formidable foe. Community-acquired MRSA has risen sharply. Presents as boils, cellulitis, or deeper infections. Treatment requires culture-guided antibiotics (trimethoprim-sulfamethoxazole, doxycycline, or vancomycin for MRSA).
Abscess: A walled-off collection of pus. The treatment is still “incision and drainage” — antibiotics alone are inadequate for a formed abscess. Packing, warm compresses, and follow-up are standard.
Wound Infections: Any breach in skin can become infected. Signs: increasing redness, warmth, purulent discharge, fever, red streaking (suggesting lymphangitis — a red flag for escalating infection). Treatment depends on depth and severity.
11. Rashes

“Rash” is a catch-all term for an enormous variety of skin changes. Contact dermatitis (allergic or irritant), drug reactions, viral exanthems, heat rash, fungal infections, and dozens of other conditions present as rashes.
Workup: History is everything. Timing, distribution, associated symptoms, recent medications, exposures. Patch testing identifies contact allergens. KOH prep identifies fungal causes.
Treatment: Entirely dependent on the underlying cause. Antihistamines and topical steroids for allergic/irritant causes. Antivirals for viral causes. Antifungals for tinea. Identifying and eliminating the trigger is paramount.
12. Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN)

Stevens Johnson Syndrome
These are medical emergencies. SJS/TEN exist on a severity spectrum — SJS involves less than 10% body surface area involvement; TEN involves more than 30%. Both involve widespread skin detachment, resembling severe burns. Mortality in TEN can reach 30–40%.

Toxic Epidermal Necrosis Syndrome (T.E.N.S.)
Causes: Overwhelmingly drug-induced (antibiotics, anticonvulsants, allopurinol, NSAIDs, sulfa drugs). Rarely, infections (Mycoplasma) trigger SJS.
Diagnosis: Clinical, confirmed by skin biopsy (full-thickness epidermal necrosis).
Treatment: ICU-level care — fluids, wound management, pain control, nutrition, ophthalmology consultation (eyes are commonly affected). Cyclosporine and IV immunoglobulin (IVIG) are used, though evidence is still evolving. Immediate cessation of the offending drug is critical. Burn units provide optimal care.
Prevention: Pharmacogenomic testing (e.g., HLA-B5701 for abacavir, HLA-B1502 for carbamazepine) can identify at-risk individuals before prescribing.
13. Psoriasis

Psoriasis affects approximately 7.5 million Americans and 125 million people worldwide. It’s far more than a skin disease — it’s a systemic inflammatory condition with cardiovascular, metabolic, and mental health implications.
Types: Plaque (most common — raised silvery-scaled plaques), guttate, inverse, pustular, erythrodermic. Psoriatic arthritis develops in up to 30% of patients.
Causes: Immune-mediated (Th17 pathway), with strong genetic component (HLA-Cw6). Triggers include stress, infections (strep), certain medications (beta-blockers, lithium), and skin trauma (Koebner phenomenon).
Diagnosis: Clinical. Biopsy when uncertain.
Treatment: A revolution has happened here. Topical steroids, vitamin D analogs, and phototherapy remain foundational. Biologic agents — TNF inhibitors (adalimumab), IL-17 inhibitors (secukinumab, ixekizumab), IL-23 inhibitors (risankizumab, guselkumab) — achieve near-complete clearance in many patients. Oral small molecules (apremilast, deucravacitinib) offer newer non-biologic options. For biohackers: dietary anti-inflammatory strategies, stress reduction, and gut microbiome optimization are documented adjuncts.
14. Eczema (Atopic Dermatitis)

Eczema affects 31 million Americans and is the most common chronic inflammatory skin disease. It often begins in childhood and can persist into adulthood — and adult-onset eczema is increasingly recognized.
Causes: A dysfunctional skin barrier (often involving filaggrin gene mutations), immune dysregulation (Th2-skewed), and environmental triggers. Part of the “atopic triad” with asthma and allergic rhinitis.
Symptoms: Intense itch (the hallmark), dry skin, red to brownish-gray patches, thickened/cracked/scaly skin. Itch-scratch cycle perpetuates the condition.
Diagnosis: Clinical. Patch testing to identify contact allergens. IgE levels and RAST testing for allergen identification.
Treatment: Moisturizers as the foundation — barrier repair is everything. Topical steroids for flares. Calcineurin inhibitors (tacrolimus, pimecrolimus) for sensitive areas. The breakthrough: dupilumab (Dupixent) — an IL-4/IL-13 inhibitor — transformed moderate-to-severe eczema management. Newer biologics (tralokinumab, lebrikizumab) and JAK inhibitors (upadacitinib, abrocitinib) are expanding options significantly. Identifying and minimizing triggers (specific allergens, irritants, heat, stress) is critical.
15. Hidradenitis Suppurativa (HS)

HS is one of the most painful, debilitating, and underdiagnosed chronic skin conditions. It affects approximately 1–4% of the population, disproportionately impacting women and people of color, and typically begins after puberty.
What it is: Recurrent, painful nodules, abscesses, and tunnels (sinus tracts) in areas where skin rubs — armpits, groin, buttocks, under the breasts. The lesions can rupture, drain, and leave significant scarring.
Causes: Follicular occlusion triggers inflammation, not infection. Hormonal influences, obesity, smoking, and genetic factors play roles. The NCSTN, PSENEN, and PSEN1 genes have been implicated. Often associated with metabolic syndrome, IBD, and depression.
Diagnosis: Clinical (Hurley staging I–III). Often misdiagnosed as recurrent boils for years.
Treatment: Antibiotics (tetracyclines, clindamycin) for mild disease. Adalimumab (Humira) is the only FDA-approved biologic for HS and achieves meaningful response in moderate-to-severe disease. Secukinumab recently received FDA approval for HS as well (2023). Surgical options — deroofing, wide excision — are used for Hurley III disease. Weight loss and smoking cessation make a measurable difference. HS communities and specialist care are invaluable; this condition has historically been undertreated and underfunded.
The Bigger Picture: Your Skin Talks, Are You Listening?
Skin conditions don’t exist in isolation. Rosacea links to gut health. Psoriasis predicts cardiovascular risk. HS connects to metabolic syndrome. Vitiligo signals broader autoimmune activity. For the biohacker, the skin is a dashboard — rich with data about what’s happening systemically.
Foundational interventions that support skin health across almost every condition: protecting from UV, managing inflammation (through diet, sleep, and stress), supporting gut and immune health, and working with a board-certified dermatologist. New biologics, JAK inhibitors, and precision medicine are rapidly transforming what’s possible. The era of “just live with it” for chronic skin conditions is ending.
Your skin is worth understanding. It’s worth treating. And it’s worth advocating for — whether that means pushing your doctor for updated treatments or building a skincare protocol that actually works for your biology.
This article is for informational purposes only and does not constitute medical advice. Always consult a board-certified dermatologist for diagnosis and treatment.

Leave a comment